The Duty Microbiologist had just got to the duty desk when the phone rang, 09:02 no time to even pour a cup of coffee… this was going to be a bad day!
The ward doctor from Phlegming Ward was treating an unknown illness in a patient who had just returned from a holiday from the Indian Subcontinent.
It sounded bad… they were septic, with low blood pressure and a very high lactate. The Critical Care Outreach Team were on their way but the team were worried the normal IV Amoxicillin, Gentamicin and Metronidazole for sepsis wasn’t working!
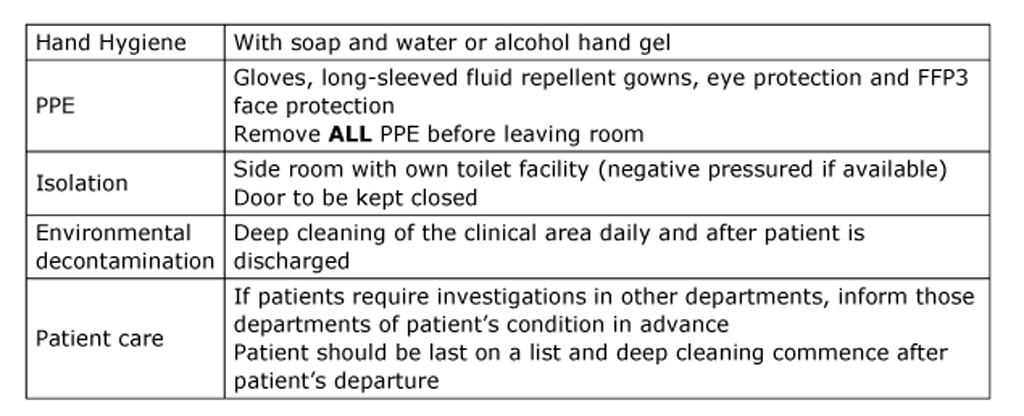
“Change to Meropenem, give a dose of Amikacin stat and isolate the patient ASAP. Also send us a blood culture, sputum and urine and we’ll see what we can grow. As there is a risk of enteric fever, make sure you write High Risk on the request form please!”
However, at the same time the Sister from Phlegming Ward was calling the Infection Control Nurses to say she thought they might have an outbreak as they had a number of patients that had all been in the same bay who were now all suddenly septic!
The Infection Control Nurses told the Sister they’d drop everything and hurry along to assess the situation; so they brought forward elevenses to a 10am cake break and then off they went… which is pretty speedy for IC! (…I am going to be in so much trouble for writing that!!!)
When they arrived on Phlegming Ward the corridor looked dark and gloomy. The overhead strip lights flickered on and off like a broken strobe light at an 80s disco. A trail of bright pink slime oozed its way across the broken floor tiles disappearing off into the distance. Nothing moved; everything was silent. The ICNs looked through the doors to see carnage. To be fair it was often a chaotic place where no one ever washed up their coffee cups, so mould outbreaks were common. They entered the ward. This seemed different; the patients looked terrible, emaciated and sunken eyed which, although food was being cut back to make hospital savings, shouldn’t be noticeable quiet yet. There was also blood and vomit everywhere, as well as some funny looking bright pink stains no one quite knew what to make of, and the over-worked staff looked like they had finally lost the plot!
The ward doctor from Phlegming Ward was treating an unknown illness in a patient who had just returned from a holiday from the Indian Subcontinent.
It sounded bad… they were septic, with low blood pressure and a very high lactate. The Critical Care Outreach Team were on their way but the team were worried the normal IV Amoxicillin, Gentamicin and Metronidazole for sepsis wasn’t working!
“Change to Meropenem, give a dose of Amikacin stat and isolate the patient ASAP. Also send us a blood culture, sputum and urine and we’ll see what we can grow. As there is a risk of enteric fever, make sure you write High Risk on the request form please!”
However, at the same time the Sister from Phlegming Ward was calling the Infection Control Nurses to say she thought they might have an outbreak as they had a number of patients that had all been in the same bay who were now all suddenly septic!
The Infection Control Nurses told the Sister they’d drop everything and hurry along to assess the situation; so they brought forward elevenses to a 10am cake break and then off they went… which is pretty speedy for IC! (…I am going to be in so much trouble for writing that!!!)
When they arrived on Phlegming Ward the corridor looked dark and gloomy. The overhead strip lights flickered on and off like a broken strobe light at an 80s disco. A trail of bright pink slime oozed its way across the broken floor tiles disappearing off into the distance. Nothing moved; everything was silent. The ICNs looked through the doors to see carnage. To be fair it was often a chaotic place where no one ever washed up their coffee cups, so mould outbreaks were common. They entered the ward. This seemed different; the patients looked terrible, emaciated and sunken eyed which, although food was being cut back to make hospital savings, shouldn’t be noticeable quiet yet. There was also blood and vomit everywhere, as well as some funny looking bright pink stains no one quite knew what to make of, and the over-worked staff looked like they had finally lost the plot!

This is real!








 RSS Feed
RSS Feed
