The Microbiology Consultant was waiting for the new Microbiology Registrar to finish the authorisation before going through any problems or questions they had. They started with their first question, a urine isolate which was identified as Pseudomonas aeruginosa but the antibiotic sensitivities didn’t make sense. The bacterium was sensitive to Co-amoxiclav and Ceftriaxone but resistant to Gentamicin and Amikacin. Pseudomonas aeruginosa is normally resistant to Co-amoxiclav and Ceftriaxone and sensitive to Gentamicin and Amikacin. A “nonsensical” or “incorrect” result like this should normally prompt further investigation as to what might be wrong before it is authorised or released.
The Registrar said, “I was going to send this back to the lab and ask them to repeat the sensitivities”.
“Wait a moment,” said the Consultant paying more attention. “Let’s have a look at the patient’s other results”.
Scanning through the other results they saw that over the past couple of weeks the patient had had 2 sets of blood cultures and 3 urines with the same bacterium isolated, and always with the same “odd” sensitivity pattern.
The Consultant started to swear! The Registrar looked at him in horror; this was very out of character.
As he finally started to calm down the Consultant said “Okay, today’s lesson is that when Pseudomonas aeruginosa looks like Pseudomonas aeruginosa but doesn’t act like Pseudomonas aeruginosa… think Burkholderia pseudomallei… this patient has meliodosis… and we now have a biological safety incident to sort out in the lab”. The swearing started all over again…
“Oops” said the Registrar but actually didn’t really know what all that meant…maybe I need a hazmat suit they thought!
What is meliodosis?
Meliodosis is caused by the bacterium Burkholderia pseudomallei, a Gram-negative bacillus that grows aerobically. The bacterium is a saprophyte (it lives on dead and decaying material in the environment), found in soil and water. It is a common infection found throughout Asia, but particularly in Thailand, Malaysia, Singapore and Northern Australia. Peaks of infection occur during the wet season. The biggest risk of transmission occurs from direct inoculation through the skin of contaminated soil and water, although occasionally it may be by inhalation. It is estimated that there are about 165,000 cases with 89,000 deaths a year from meliodosis worldwide. The incubation period is said to be up to 21 days however it is possible for an asymptomatic carrier to develop infection many years after initial colonisation (up to 25 years in some studies).
How does meliodosis present?
Meliodosis can present in numerous ways:
The mortality from meliodosis is up to 40% even with appropriate treatment. Risk factors for more severe infection include diabetes mellitus, alcoholism, chronic renal disease and chronic lung disease.
How is B. pseudomallei identified?
In the past it was difficult for laboratories to identify B. pseudomallei. This was because young colonies look like a normal Pseudomonas aeruginosa on blood and CLED agar, they are oxidase positive like P. aeruginosa added to this the biochemical API identification method misidentifies it as P. aeruginosa. It was therefore very easy to report out the wrong organism and miss the significance of the culture. In fact up until 1992 B. pseudomallei was actually called Pseudomonas pseudomallei.
“Wait a moment,” said the Consultant paying more attention. “Let’s have a look at the patient’s other results”.
Scanning through the other results they saw that over the past couple of weeks the patient had had 2 sets of blood cultures and 3 urines with the same bacterium isolated, and always with the same “odd” sensitivity pattern.
The Consultant started to swear! The Registrar looked at him in horror; this was very out of character.
As he finally started to calm down the Consultant said “Okay, today’s lesson is that when Pseudomonas aeruginosa looks like Pseudomonas aeruginosa but doesn’t act like Pseudomonas aeruginosa… think Burkholderia pseudomallei… this patient has meliodosis… and we now have a biological safety incident to sort out in the lab”. The swearing started all over again…
“Oops” said the Registrar but actually didn’t really know what all that meant…maybe I need a hazmat suit they thought!
What is meliodosis?
Meliodosis is caused by the bacterium Burkholderia pseudomallei, a Gram-negative bacillus that grows aerobically. The bacterium is a saprophyte (it lives on dead and decaying material in the environment), found in soil and water. It is a common infection found throughout Asia, but particularly in Thailand, Malaysia, Singapore and Northern Australia. Peaks of infection occur during the wet season. The biggest risk of transmission occurs from direct inoculation through the skin of contaminated soil and water, although occasionally it may be by inhalation. It is estimated that there are about 165,000 cases with 89,000 deaths a year from meliodosis worldwide. The incubation period is said to be up to 21 days however it is possible for an asymptomatic carrier to develop infection many years after initial colonisation (up to 25 years in some studies).
How does meliodosis present?
Meliodosis can present in numerous ways:
- Pneumonia, either acute or chronic mimicking tuberculosis
- Skin ulcers and abscesses
- Prostatitis and prostatic abscess
- Abscesses in liver, spleen and kidneys
- Chronic osteomyelitis and septic arthritis
- Meningoencephalitis (only seen in Northern Australia)
- Parotitis (only seen in children in Thailand and Cambodia)
- Septicaemia
- Asymptomatic colonisation, detected when sending samples to the laboratory for other reasons e.g. sputum
The mortality from meliodosis is up to 40% even with appropriate treatment. Risk factors for more severe infection include diabetes mellitus, alcoholism, chronic renal disease and chronic lung disease.
How is B. pseudomallei identified?
In the past it was difficult for laboratories to identify B. pseudomallei. This was because young colonies look like a normal Pseudomonas aeruginosa on blood and CLED agar, they are oxidase positive like P. aeruginosa added to this the biochemical API identification method misidentifies it as P. aeruginosa. It was therefore very easy to report out the wrong organism and miss the significance of the culture. In fact up until 1992 B. pseudomallei was actually called Pseudomonas pseudomallei.
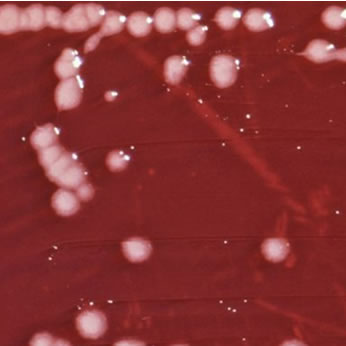
Pseudomonas aeruginosa
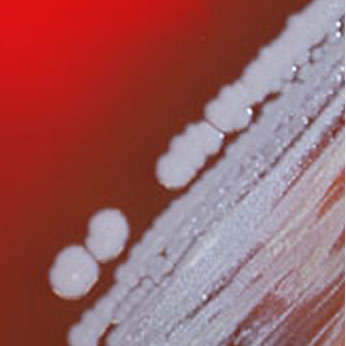
Burkholderia pseudomallei
B. pseudomallei does not have a normal P. aeruginosa sensitivity panel. The trick to identifying this bacterium is to spot the unusual antibiotic sensitivity pattern. In terms of the common anti-Gram-negative antibiotics the differences are shown in the table below; it was these paradoxical results that alerted Microbiologist to the possibility of B. pseudomallei.
Antibiotic |
P. aeruginosa |
B. pseudomallei |
Co-amoxiclav, Ceftriaxone, Cefotaxime |
Resistant |
Sensitive |
Gentamicin, Amikacin, Tobramycin, Colistin |
Sensitive |
Resistant |
Fortunately for many laboratories new methods of bacterial identification, such as matrix assisted laser desorption/ionisation time of flight (MALDI-TOF), have put an end to the difficulties of identifying B. pseudomallei. However if you are still reliant on biochemical APIs then both Biomedical Scientists and Microbiologists need to be vigilant for these seemingly “wrong” sensitivity patterns and take action.
Serology looking for antibodies against B. pseudomallei can be helpful in diagnosing infection in patients who are not from endemic countries. It is less helpful for proving infection in patients from endemic areas as past exposure gives positive serology, therefore asymptomatic infection and chronic colonisation can both give positive results in the absence of infection. However, if the patient is not from an endemic country and does have positive serology, then this helps to prove infection.
Laboratory implications
B. pseudomallei is a Biological Safety Category 3 microorganism and as such should only be handled in a Category 3 facility such as that used to process respiratory and tuberculosis specimens. Unfortunately, due to problems with identification in the past, cultures of B. pseudomallei have been processed on the open bench putting laboratory staff at risk of infection and colonisation. This is often because there were insufficient clinical details on the specimen request cards!! Factor in the high mortality rate and the potentially long incubation period from exposure to infection and you can see that mishandling this bacterium poses a major risk to people’s safety.
Serology looking for antibodies against B. pseudomallei can be helpful in diagnosing infection in patients who are not from endemic countries. It is less helpful for proving infection in patients from endemic areas as past exposure gives positive serology, therefore asymptomatic infection and chronic colonisation can both give positive results in the absence of infection. However, if the patient is not from an endemic country and does have positive serology, then this helps to prove infection.
Laboratory implications
B. pseudomallei is a Biological Safety Category 3 microorganism and as such should only be handled in a Category 3 facility such as that used to process respiratory and tuberculosis specimens. Unfortunately, due to problems with identification in the past, cultures of B. pseudomallei have been processed on the open bench putting laboratory staff at risk of infection and colonisation. This is often because there were insufficient clinical details on the specimen request cards!! Factor in the high mortality rate and the potentially long incubation period from exposure to infection and you can see that mishandling this bacterium poses a major risk to people’s safety.

So what if a Category 3 facility wasn’t used?
After wrestling the Registrar out of a hazmat suit, the first step is to:
How might laboratory staff identify B. pseudomallei?
The key to identifying B. pseudomallei is to be aware of when results don’t fit with what you expect to see, which with this bacterium is when a supposed Pseudomonas spp. doesn’t have the normal Pseudomonas spp. antibiotic sensitivities. In particular, a Pseudomonas spp. that is sensitive to Co-amoxiclav and Ceftriaxone and resistant to Gentamicin and Amikacin should start to ring alarm bells! If you think you might have B. pseudomallei then do any further work with the bacterium in a Category 3 facility. Also immediately identify any other specimens from that patient and ensure they are all processed from then on as HIGH RISK!
How is meliodosis treated?
There are two phases in the treatment of meliodosis. The initial phase treats the acute infection and the follow-up phase eradicates carriage of B. pseudomallei.
After wrestling the Registrar out of a hazmat suit, the first step is to:
- Quarantine all specimens from that patient and make sure these are only processed in a Category 3 facility from then on.
- Next make a list of all members of staff who have been involved in processing these samples, especially those who have handled pure cultures. All of these members of staff should be made known to the Occupational Health Department. Serological blood tests can be performed acutely then at 1 month and 3 months to look to see if any member of staff seroconverts, indicating early infection or acquisition, but serology can be negative in the context of colonisation. Staff can be offered prophylaxis with either Co-trimoxazole or Co-amoxiclav for 21 days although there is no firm evidence that this definitely prevents infection.
- All told, dealing with these types of incidents is both time consuming and causes a lot of anxiety for exposed and “at risk” laboratory staff…do me a favour… FILL OUT FORMS CORRECTLY!
How might laboratory staff identify B. pseudomallei?
The key to identifying B. pseudomallei is to be aware of when results don’t fit with what you expect to see, which with this bacterium is when a supposed Pseudomonas spp. doesn’t have the normal Pseudomonas spp. antibiotic sensitivities. In particular, a Pseudomonas spp. that is sensitive to Co-amoxiclav and Ceftriaxone and resistant to Gentamicin and Amikacin should start to ring alarm bells! If you think you might have B. pseudomallei then do any further work with the bacterium in a Category 3 facility. Also immediately identify any other specimens from that patient and ensure they are all processed from then on as HIGH RISK!
How is meliodosis treated?
There are two phases in the treatment of meliodosis. The initial phase treats the acute infection and the follow-up phase eradicates carriage of B. pseudomallei.
Initial acute infection |
IV Ceftazidime 2g TDS OR IV Meropenem 1g TDS |
Eradication |
PO Co-trimoxazole 2x960mg BD* OR PO Co-amoxiclav 3x625mg TDS* |
*Note, these are much higher doses than normal conventional licensed doses
Duration
The relapse rate following “adequate” treatment is up to 10% so ensure follow-up on patients after treatment and advise them to seek medical help if they start to feel unwell again.
Infection control precautions
Despite the high risk nature of B. pseudomallei in the laboratory setting normal universal precautions can be used when caring for patients on the ward. This is because person-to-person transmission is uncommon and the amount of bacteria that the patient will be shedding into the environment is very low as opposed to a pure culture of bacteria in the laboratory.
The Microbiology Consultant and Registrar went to see the patient on the ward. On further questioning it turned out that the patient had spent the first 20 years of their life living in Thailand. During this time they had become colonised with B. pseudomallei. When they had recently developed pneumonia and become septic it was the B. pseudomallei, which was now a part of their normal flora, that had got into the chest and caused the infection. The patient was put on IV Meropenem and slowly improved. After two weeks of Meropenem they were switched to the eradication therapy, Co-trimoxazole, and went home.
Twenty one laboratory staff exposed to B. pseudomallei were identified and bloods were taken for serology. All exposed staff were given prophylactic antibiotics and none of them seroconverted or became colonised with the bacterium. On further investigation it became clear that none of the laboratory staff had ever seen B. pseudomallei before, which is understandable in the UK where this bacterium is only seen rarely. The important lesson for everyone was that if a bacterium is not behaving in a way you would normally expect then don’t just accept the results but ask someone senior what might be going on and think about why it might be happening. This particular episode was a lucky escape but it could have been much worse if lab staff had developed meliodosis.
The Registrar also learnt some valuable lessons in microbiology as well as a few new swear words… both might come in handy in the future!
Reference
Treatment and prophylaxis of meliodosis. Dance, D. Int J Antimicrob Agents 2014, 43(4), 310-18
Duration
- Pneumonia, skin abscesses, septicaemia with no deep focus – 2 weeks initial PLUS 3 months eradication
- Prostatic or other deep abscess and septic arthritis – 4 weeks initial PLUS 3 months eradication
- Osteomyelitis – 6 weeks initial PLUS 6 months eradication
- Neurological – 8 weeks initial PLUS 6 months eradication
The relapse rate following “adequate” treatment is up to 10% so ensure follow-up on patients after treatment and advise them to seek medical help if they start to feel unwell again.
Infection control precautions
Despite the high risk nature of B. pseudomallei in the laboratory setting normal universal precautions can be used when caring for patients on the ward. This is because person-to-person transmission is uncommon and the amount of bacteria that the patient will be shedding into the environment is very low as opposed to a pure culture of bacteria in the laboratory.
The Microbiology Consultant and Registrar went to see the patient on the ward. On further questioning it turned out that the patient had spent the first 20 years of their life living in Thailand. During this time they had become colonised with B. pseudomallei. When they had recently developed pneumonia and become septic it was the B. pseudomallei, which was now a part of their normal flora, that had got into the chest and caused the infection. The patient was put on IV Meropenem and slowly improved. After two weeks of Meropenem they were switched to the eradication therapy, Co-trimoxazole, and went home.
Twenty one laboratory staff exposed to B. pseudomallei were identified and bloods were taken for serology. All exposed staff were given prophylactic antibiotics and none of them seroconverted or became colonised with the bacterium. On further investigation it became clear that none of the laboratory staff had ever seen B. pseudomallei before, which is understandable in the UK where this bacterium is only seen rarely. The important lesson for everyone was that if a bacterium is not behaving in a way you would normally expect then don’t just accept the results but ask someone senior what might be going on and think about why it might be happening. This particular episode was a lucky escape but it could have been much worse if lab staff had developed meliodosis.
The Registrar also learnt some valuable lessons in microbiology as well as a few new swear words… both might come in handy in the future!
Reference
Treatment and prophylaxis of meliodosis. Dance, D. Int J Antimicrob Agents 2014, 43(4), 310-18
 RSS Feed
RSS Feed
