One of my biggest concerns around the current Covid-19 pandemic is that all of the normal things that make people sick haven’t gone away. This concerns me because whilst Covid-19 is on the minds of healthcare staff they may inadvertently delay considering all of the other clinical problems that will continue to be going on in the background. Patients will still be coming in with appendicitis, UTIs, heart attacks and strokes; in fact ANY acute medical or surgical problem that happens in a normal day in the NHS.

One area where I think this could become a major issue is sepsis. Now I know I’m a Microbiologist and we’re always banging on about sepsis but there are good reasons for this:
- Sepsis kills
- Healthcare workers find it difficult to recognise sepsis, even on a normal day, and therefore treatment can be delayed
- Delaying effective treatment results in more of No. 1

Click for larger image
What is sepsis?
Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is sepsis with circulatory, cellular or metabolic dysfunction, and has a high mortality.
Almost any bacterium can cause sepsis although the most common culprits are:
Sepsis and septic shock are clinical diagnoses not laboratory diagnoses:
Sepsis and septic shock are medical emergencies and early recognition and treatment improve survival.
The main risk factors for sepsis are:
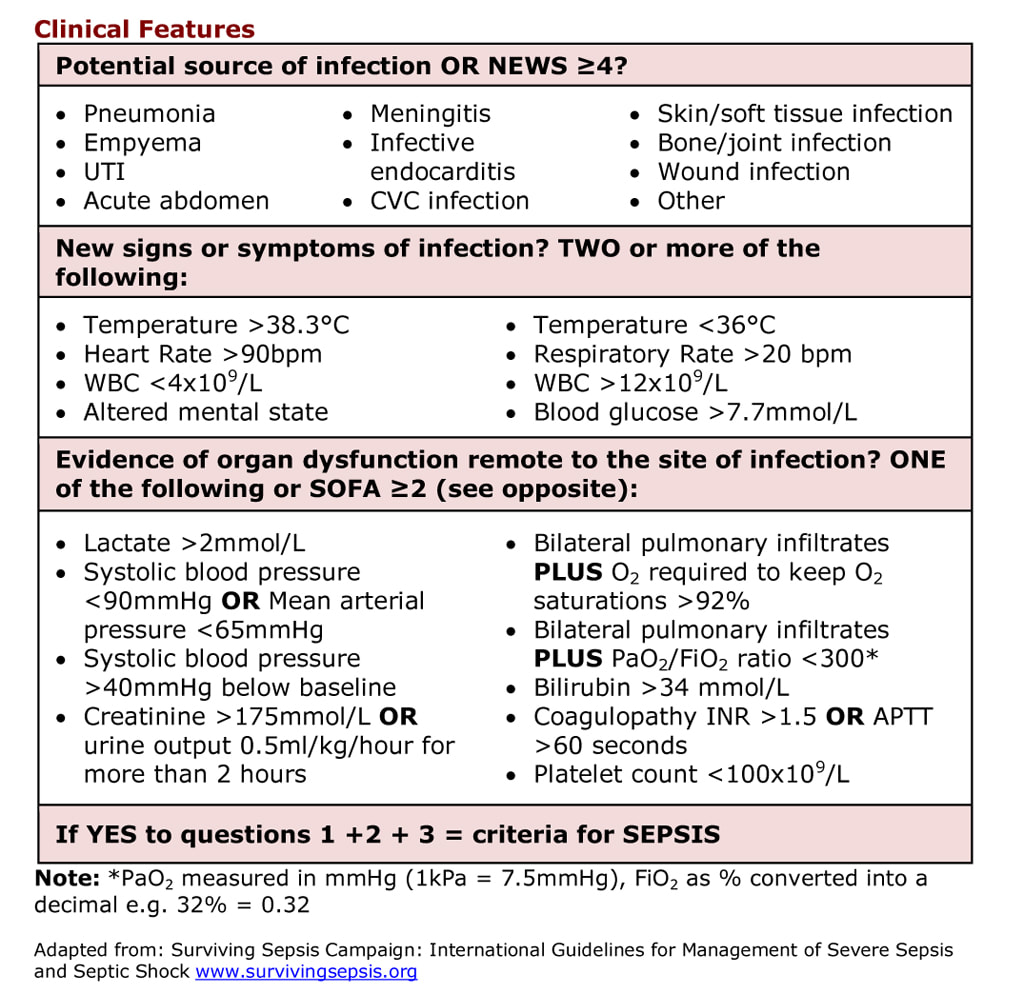
What are the clinical features of sepsis
Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is sepsis with circulatory, cellular or metabolic dysfunction, and has a high mortality.
Almost any bacterium can cause sepsis although the most common culprits are:
- Staphylococcus aureus
- Group A Beta-haemolytic Streptococcus
- Enterobacteriaceae e.g. Escherichia coli, Klebsiella spp., Enterobacter spp.,
- Pseudomonas spp.
- Neisseria meningitidis
Sepsis and septic shock are clinical diagnoses not laboratory diagnoses:
- Sepsis - infection with evidence of a systemic response to that infection e.g. hypoxia, oliguria, confusion
- Septic shock - sepsis associated with organ dysfunction, hypoperfusion or hypotension
Sepsis and septic shock are medical emergencies and early recognition and treatment improve survival.
The main risk factors for sepsis are:
- Age <1 year or >75 years
- Frailty or comorbidities e.g. diabetes, renal failure, liver failure
- Trauma, surgery or other invasive procedure within 6 weeks
- Immunosuppression
- Intravascular device
- Breaches to skin integrity e.g. cuts, burns, blisters
- Current or recent pregnancy (within 6 weeks)
What are the clinical features of sepsis
Click for larger image
NEWS is a National Early Warning Score, a set of measurements that alert ward staff to a deteriorating patient who needs review by a doctor.

Click for larger image
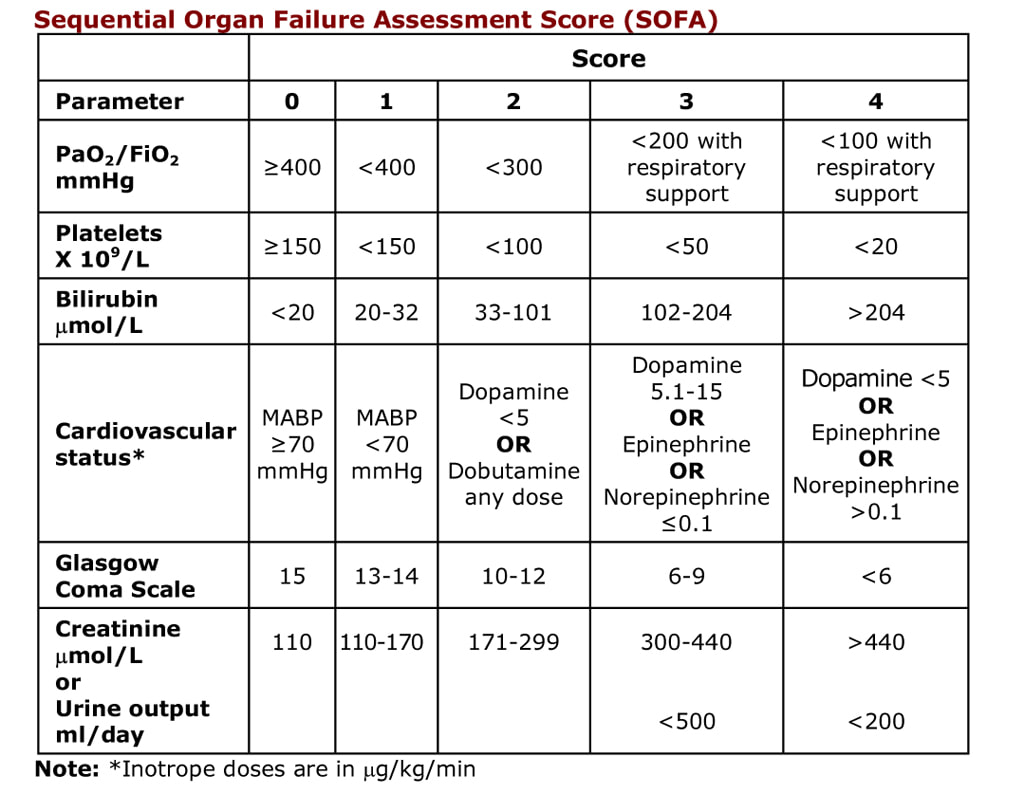
Why not use the SOFA scoring system?
SOFA is the Sequential Organ Failure Assessment score. It is a clinical scoring system used in medicine to predict the severity of an illness and help guide the amount of supportive care a patient might need e.g. ITU admission. The SOFA score is objective and reproducible BUT it is based upon lab tests and infusion parameters and so in my opinion is of limited value in diagnosing sepsis in the acute setting as it can take too long to get these results back. The “Surviving Sepsis” scoring system above still has lab results but in my opinion it also has an enough criteria to help with a more rapid diagnosis of sepsis.
SOFA is the Sequential Organ Failure Assessment score. It is a clinical scoring system used in medicine to predict the severity of an illness and help guide the amount of supportive care a patient might need e.g. ITU admission. The SOFA score is objective and reproducible BUT it is based upon lab tests and infusion parameters and so in my opinion is of limited value in diagnosing sepsis in the acute setting as it can take too long to get these results back. The “Surviving Sepsis” scoring system above still has lab results but in my opinion it also has an enough criteria to help with a more rapid diagnosis of sepsis.
Click for larger image

Click for larger image
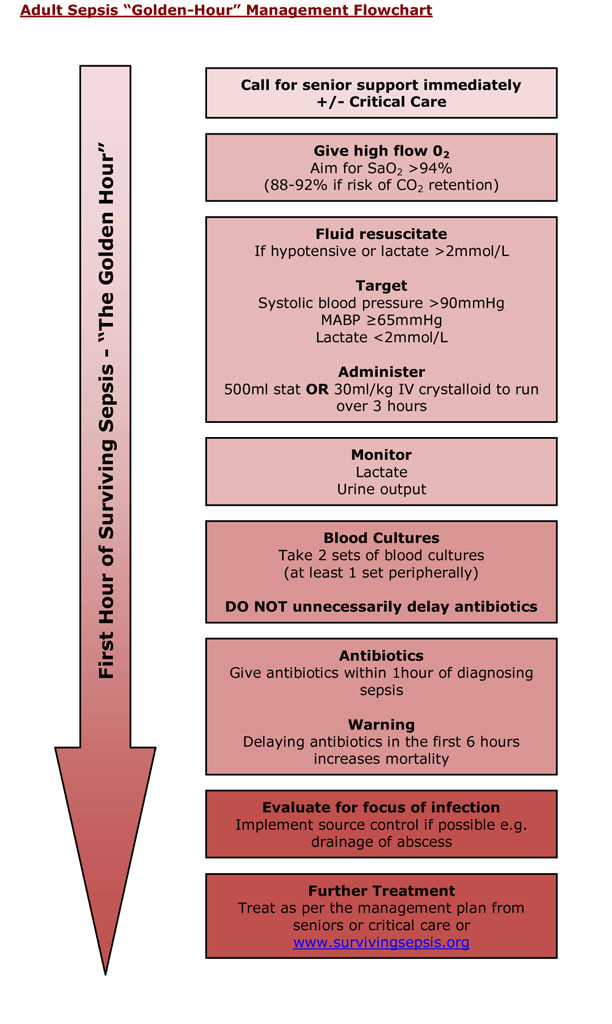
How is sepsis treated?
Antibiotics should be given within 1 hour of the diagnosis of sepsis so waiting until the Covid-19 test result comes back will be too late as it takes a lot longer to get a SARS Cov2 result.
My personal antibiotic preferences for treating sepsis are below; however you should follow your own hospitals guidelines if they are available. Remember: these antibiotics are for when the source of infection is unclear, they are empirical guidelines. If you know the source of someone’s sepsis then you should treat for that e.g. community acquired pneumonia, pyelonephritis, cellulitis, etc.
Empirical guidelines for sepsis in adults
Antibiotics should be given within 1 hour of the diagnosis of sepsis so waiting until the Covid-19 test result comes back will be too late as it takes a lot longer to get a SARS Cov2 result.
My personal antibiotic preferences for treating sepsis are below; however you should follow your own hospitals guidelines if they are available. Remember: these antibiotics are for when the source of infection is unclear, they are empirical guidelines. If you know the source of someone’s sepsis then you should treat for that e.g. community acquired pneumonia, pyelonephritis, cellulitis, etc.
Empirical guidelines for sepsis in adults
1st line |
IV Piptazobactam PLUS IV Gentamicin |
2nd line (if 1st line contraindicated) |
IV Teicoplanin OR IV Vancomycin PLUS IV Gentamicin PLUS IV Metronidazole |
If previous ESBL or AmpC positive bacteria |
IV Meropenem PLUS IV Gentamicin |
If MRSA positive |
ADD IV Teicoplanin OR IV Vancomycin |
In addition to QUICK administration of antibiotics the source of sepsis should be identified and managed as soon as possible e.g. removal of infected CVC, drainage of abscess, repair of perforated abdominal viscus.
Click for larger image
So what does this mean in the Covid-19 pandemic?
Basically, if you see a febrile patient who you think might have Covid-19 look for signs of sepsis and if they are present then make sure you treat for sepsis whilst you are waiting for your Covid-19 tests to come back. All sick Covid-19 patients’ will fulfil some of the sepsis criteria (temperature >38.3°C, respiratory rate >20 bpm and bilateral pulmonary infiltrates) however not every Covid-19 patient is going to be septic… BUT if you look for and identify a septic patient, treat the sepsis. You don’t have to treat every Covid-19 patient for sepsis… just those who are septic!
That way you are less likely to miss an alternative diagnosis to Covid-19 and your patients will be safer amidst all of the Covid-19 distractions.
Basically, if you see a febrile patient who you think might have Covid-19 look for signs of sepsis and if they are present then make sure you treat for sepsis whilst you are waiting for your Covid-19 tests to come back. All sick Covid-19 patients’ will fulfil some of the sepsis criteria (temperature >38.3°C, respiratory rate >20 bpm and bilateral pulmonary infiltrates) however not every Covid-19 patient is going to be septic… BUT if you look for and identify a septic patient, treat the sepsis. You don’t have to treat every Covid-19 patient for sepsis… just those who are septic!
That way you are less likely to miss an alternative diagnosis to Covid-19 and your patients will be safer amidst all of the Covid-19 distractions.

 RSS Feed
RSS Feed
