It was another dull and dreary afternoon giving advice when an excited Dermatologist phoned about a patient with funny skin lumps. (Microbiologists get excited about bugs, Dermatologists get excited about rashes, so lumps and bumps together… what can I say…we were very excited!!)
Their patient was a keen gardener who had been clearing a large number of blackthorn trees (good for making sloe gin) and despite wearing thick gloves had managed to get pricked and scratched all the way up their arms. At the site of one of those puncture wounds they had developed a small red lump which had eventually turned into a small ulcer. The ulcer hadn’t got much better and over the next few weeks the patient had noticed a number of other lumps appearing up their arm and then hard swellings in their armpit.
Their patient was a keen gardener who had been clearing a large number of blackthorn trees (good for making sloe gin) and despite wearing thick gloves had managed to get pricked and scratched all the way up their arms. At the site of one of those puncture wounds they had developed a small red lump which had eventually turned into a small ulcer. The ulcer hadn’t got much better and over the next few weeks the patient had noticed a number of other lumps appearing up their arm and then hard swellings in their armpit.

Both the patient and their family Doctor thought they might have an aggressive skin cancer which had spread to the lymph nodes but the Dermatologist thought this might be something else.
“I think this might be sporotrichosis” said the Dermatologist.
The Microbiologist nearly fell off his chair! What a great piece of clinical acumen he thought; this could indeed be sporotrichosis.
“How the heck did you think of that?” the Microbiologist asked.
“Oh, I’ve seen it before when I worked in Brazil for a while” answered the Dermatologist. “But I can’t remember how to diagnose it or treat it…!”
Crikey, thought the Microbiologist, not sure I would even have thought of it…
So what is sporotrichosis?
Sporotrichosis is a sub-acute or chronic infection caused by the fungus Sporothrix schenkii. Laboratories tend to identify S. schenkii but in fact there are actually a group of at least six different fungi, the most common of which is S. schenkii. Others in the group include S. brasiliensis, S. globosa, S. mexicana, S luriei and S. pallida. Sporotrichosis is very rare in the UK with only 1 case report in the literature since the year 2000.
Where do you find S. schenkii?
Sporothrix schenkii occurs Worldwide, and is found in organic matter such as sphagnum moss, hay, soil and other vegetation. Most cases of sporotrichosis have occurred in Brazil, USA, India, Japan and Mexico. It occurs in people who have occupational exposure to these sources of fungi such as gardeners, farmers, landscapers and even Christmas tree sales people! Infection can occur when the fungal spores are inoculated through the skin or when a wound is contaminated with organic material.
An outbreak of 84 cases of sporotrichosis, in Wisconsin in the USA, occurred due to contaminated sphagnum moss used to pack conifer seedlings. In South Africa in the 1960s there were over 3000 cases due to exposure to splinters from contaminated timber used in gold mining.
In Rio de Janiero, Brazil, there is a very large on-going outbreak of sporotrichosis due to S. brasiliensis, where more than 2,000 cases have occurred since 1988 spread from infected domestic cats. The cats have had a mixture of skin and respiratory infections, which has spread to their owners mainly via facial and mucus membrane involvement (another reason not to kiss your cat!).
There have also been a few cases of laboratory acquired sporotrichosis described in the literature where lab workers have caught the infection from handling either cultures of the mould form or infected animals.
How does sporotrichosis present?
Most cases of sporotrichosis are lymphocutaenous and follow inoculation of spores into soft tissue in patients who are otherwise fit and healthy. A papule (a small lump up to 1cm in diameter) forms within days to weeks at the original point of entry and eventually ulcerates, develops surrounding redness (erythema) and discharges clear colourless and odourless fluid. Over the next few weeks further skin lesions develop along the line of lymphatic drainage in a process known as “sporotrichoid spread” with enlargement of the associated lymph nodes. Without treatment the lesions will persist indefinitely with periods of improvement followed by flare-ups; even without treatment this form of infection is not fatal.
Sporotrichosis can also occur as an opportunistic infection in patients with other underlying illnesses:
How is sporotrichosis diagnosed?
A history of exposure to potentially contaminated organic material is the key to making the diagnosis along with the typical pattern of cutaneous sporotrichoid spread.
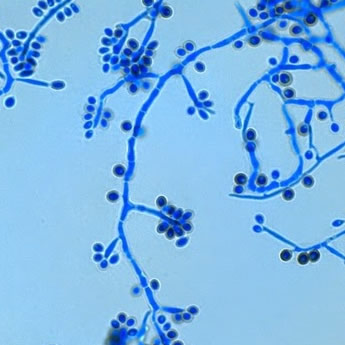
The gold standard way of diagnosing sporotrichosis is to grow the fungus from tissue or body fluid. Sporothrix spp. are dimorphic fungi; they have two different growth characteristics depending on the temperature at which they are growing. At environmental temperatures around 25-30oC they grow as a filamentous mould whereas at body temperature they grow as a yeast. The mould takes 1-2 weeks to become apparent and then grows to form cream coloured colonies which eventually turn grey and produce the typical fluffy mycelia of a mould. The yeast form produces colonies which are cream coloured and wrinkled. Once the organism is growing in the mould form it can be identified from the microscopic appearance of its mycelia, conidia and spores.
“I think this might be sporotrichosis” said the Dermatologist.
The Microbiologist nearly fell off his chair! What a great piece of clinical acumen he thought; this could indeed be sporotrichosis.
“How the heck did you think of that?” the Microbiologist asked.
“Oh, I’ve seen it before when I worked in Brazil for a while” answered the Dermatologist. “But I can’t remember how to diagnose it or treat it…!”
Crikey, thought the Microbiologist, not sure I would even have thought of it…
So what is sporotrichosis?
Sporotrichosis is a sub-acute or chronic infection caused by the fungus Sporothrix schenkii. Laboratories tend to identify S. schenkii but in fact there are actually a group of at least six different fungi, the most common of which is S. schenkii. Others in the group include S. brasiliensis, S. globosa, S. mexicana, S luriei and S. pallida. Sporotrichosis is very rare in the UK with only 1 case report in the literature since the year 2000.
Where do you find S. schenkii?
Sporothrix schenkii occurs Worldwide, and is found in organic matter such as sphagnum moss, hay, soil and other vegetation. Most cases of sporotrichosis have occurred in Brazil, USA, India, Japan and Mexico. It occurs in people who have occupational exposure to these sources of fungi such as gardeners, farmers, landscapers and even Christmas tree sales people! Infection can occur when the fungal spores are inoculated through the skin or when a wound is contaminated with organic material.
An outbreak of 84 cases of sporotrichosis, in Wisconsin in the USA, occurred due to contaminated sphagnum moss used to pack conifer seedlings. In South Africa in the 1960s there were over 3000 cases due to exposure to splinters from contaminated timber used in gold mining.
In Rio de Janiero, Brazil, there is a very large on-going outbreak of sporotrichosis due to S. brasiliensis, where more than 2,000 cases have occurred since 1988 spread from infected domestic cats. The cats have had a mixture of skin and respiratory infections, which has spread to their owners mainly via facial and mucus membrane involvement (another reason not to kiss your cat!).
There have also been a few cases of laboratory acquired sporotrichosis described in the literature where lab workers have caught the infection from handling either cultures of the mould form or infected animals.
How does sporotrichosis present?
Most cases of sporotrichosis are lymphocutaenous and follow inoculation of spores into soft tissue in patients who are otherwise fit and healthy. A papule (a small lump up to 1cm in diameter) forms within days to weeks at the original point of entry and eventually ulcerates, develops surrounding redness (erythema) and discharges clear colourless and odourless fluid. Over the next few weeks further skin lesions develop along the line of lymphatic drainage in a process known as “sporotrichoid spread” with enlargement of the associated lymph nodes. Without treatment the lesions will persist indefinitely with periods of improvement followed by flare-ups; even without treatment this form of infection is not fatal.
Sporotrichosis can also occur as an opportunistic infection in patients with other underlying illnesses:
- Pulmonary infection can occur in patients with chronic obstructive pulmonary disease (COPD) and presents in a similar fashion to tuberculosis with fever, night sweats, weight loss, worsening shortness of breath and ultimately death if untreated.
- Bone and joint (osteoarticular) infection can occur in alcoholics as a result of haematogenous spread (although rarely it can also occur via direct inoculation); bone destruction is progressive causing substantial deformity.
- Meningitis and disseminated infection can very rarely occur in profoundly immunosuppressed patients with HIV or lymphoma.
How is sporotrichosis diagnosed?
A history of exposure to potentially contaminated organic material is the key to making the diagnosis along with the typical pattern of cutaneous sporotrichoid spread.
The gold standard way of diagnosing sporotrichosis is to grow the fungus from tissue or body fluid. Sporothrix spp. are dimorphic fungi; they have two different growth characteristics depending on the temperature at which they are growing. At environmental temperatures around 25-30oC they grow as a filamentous mould whereas at body temperature they grow as a yeast. The mould takes 1-2 weeks to become apparent and then grows to form cream coloured colonies which eventually turn grey and produce the typical fluffy mycelia of a mould. The yeast form produces colonies which are cream coloured and wrinkled. Once the organism is growing in the mould form it can be identified from the microscopic appearance of its mycelia, conidia and spores.
Yeast forms of the fungus can sometimes be seen on histopathological examination of tissue, especially if using specific fungal stains, although they are not distinctive in appearance.
How is sporotrichosis treated?
The treatment of sporotrichosis depends on the type of infection.
IV liposomal Amphotericin B is incredibly expensive; in the UK AmBisome costs £575 per day to treat a 70kg patient (and many of our patients weigh much more than this!). Alternatively patients may be given the more toxic but cheaper Amphotericin B deoxycholate (Fungizone) at 0.7-1mg/kg costing just £3.88 per day for a 70kg patient… but it is very nephrotoxic!
So our patient had a biopsy taken and yeast like fungi were seen on histological examination. Two weeks later a fluffy mould was growing on culture and the laboratory was able to confirm sporotrichosis. In the meantime the patient had been empirically treated with Itraconazole and got much better; they had also decided not to do any more gardening without better protection… although a good homemade sloe gin made from the fruit of the vicious blackthorn could possibly be worth the risk!!
A tried and tested sloe gin recipe (it’s very good but please drink responsibly!!)
How is sporotrichosis treated?
The treatment of sporotrichosis depends on the type of infection.
- For lymphocutaenous infection the treatment of choice is PO Itraconazole 200mg OD until 4 weeks after all of the lesions have resolved (usually 3-6 months).
- For pulmonary, osteoarticular and disseminated sporotrichosis treatment should be started with IV liposomal Amphotericin B 3-5mg/kg OD and when the patient has shown sustained improvement they can be changed to PO Itraconazole 200mg BD for 12 months.
- Meningitis is treated with 4-6 weeks of IV liposomal Amphotericin B 3-5mg/kg OD before changing to PO Itraconazole 200mg BD for 12 months.
IV liposomal Amphotericin B is incredibly expensive; in the UK AmBisome costs £575 per day to treat a 70kg patient (and many of our patients weigh much more than this!). Alternatively patients may be given the more toxic but cheaper Amphotericin B deoxycholate (Fungizone) at 0.7-1mg/kg costing just £3.88 per day for a 70kg patient… but it is very nephrotoxic!
So our patient had a biopsy taken and yeast like fungi were seen on histological examination. Two weeks later a fluffy mould was growing on culture and the laboratory was able to confirm sporotrichosis. In the meantime the patient had been empirically treated with Itraconazole and got much better; they had also decided not to do any more gardening without better protection… although a good homemade sloe gin made from the fruit of the vicious blackthorn could possibly be worth the risk!!
A tried and tested sloe gin recipe (it’s very good but please drink responsibly!!)
- 1.2Kg cleaned and frosted or pricked sloes (Blackthorn berries)
- 120g granulated sugar (more if you want it sweeter)
- 1.6L gin (cheap as you like!)
 RSS Feed
RSS Feed
