What is long Covid?
It might surprise you to know that there is still no formal definition of long Covid, even though the term has been used a lot in both the media and scientific literature over the past 6 months or more. Long Covid is the term commonly used to describe the persistence of symptoms in a person who has had Covid-19 infection and “should have got better”, but in whom symptoms persist. However, there is no consensus on what these symptoms are or how long they must be present before they constitute long Covid. Channel 4’s Dispatches, aired on 16th March, reported from Bradford one of the country’s worst hit Covid-19 regions and gave a glimpse into the lives of some people suffering the after effects of Covid-19.
In the National Institute for Health and Care Excellence (NICE) guideline for managing the long-term effects of Covid-19 they refer to long Covid as “the persistence of symptoms or signs of Covid-19 more than 4 weeks after the initial illness”, with the caveat that there isn’t another explanation for the patients symptoms or signs. However other groups, such as the Office for National Statistics (ONS) use 5 weeks as the lower limit of time.
Well, we can’t agree on a time scale, surely we can agree what the symptoms are… can’t we?
It might surprise you to know that there is still no formal definition of long Covid, even though the term has been used a lot in both the media and scientific literature over the past 6 months or more. Long Covid is the term commonly used to describe the persistence of symptoms in a person who has had Covid-19 infection and “should have got better”, but in whom symptoms persist. However, there is no consensus on what these symptoms are or how long they must be present before they constitute long Covid. Channel 4’s Dispatches, aired on 16th March, reported from Bradford one of the country’s worst hit Covid-19 regions and gave a glimpse into the lives of some people suffering the after effects of Covid-19.
In the National Institute for Health and Care Excellence (NICE) guideline for managing the long-term effects of Covid-19 they refer to long Covid as “the persistence of symptoms or signs of Covid-19 more than 4 weeks after the initial illness”, with the caveat that there isn’t another explanation for the patients symptoms or signs. However other groups, such as the Office for National Statistics (ONS) use 5 weeks as the lower limit of time.
Well, we can’t agree on a time scale, surely we can agree what the symptoms are… can’t we?

Some things are born to be long and short!
What are the symptoms of long Covid?
The NICE guideline states that:
“Symptoms after acute Covid-19 are highly variable and wide-ranging. The most commonly reported include (but are not limited to) the following:”
So essentially almost any symptoms can occur after Covid-19! In the small number of clinical studies looking at long Covid the most common symptoms are fatigue, cough, headache, loss of sense of smell or taste and muscle pain. But there should be a caveat here too and that is that those are usually the symptoms “asked about” in those studies and so any other symptoms could be missed, and the results become biased.
It is also difficult to identify which of the symptoms are due to some form of long-term disease, i.e. long Covid, and which are due to damage caused during the acute illness (e.g. breathlessness and cough following a severe lung infection) and which are due to the psychological trauma of being very sick and in a Critical Care Unit (e.g. cognitive impairment, sleep disturbance, depression and anxiety). All are valid symptoms but not necessarily due to the “virus” itself, but more the consequences of having had the virus.
How common is long Covid?
Long Covid appears to be common. The latest figures from the ONS suggest that 22.1% of patients still have symptoms at 5 weeks, and 9.8% still have symptoms at 12 weeks. That’s huge! In the UK we have had 4.26 million cases with 126,000 deaths. That means that there are 4.134 million Covid-19 survivors in the UK, which extrapolates to about 400,000 people who still had symptoms 12 weeks after acute Covid-19!
Long Covid is also more common in females, those aged 35-49 years and the obese. In particular long Covid is more common in the main working age groups, and therefore the socio-economic impact of long Covid-19, both on the individual as well as society, could be equally huge. And yet it has attracted little research so far. This seems short-sighted to me; the more we know about it the better we should be at managing it.
What is the cause of long Covid?
Guess what? No one agrees as no one knows!!!! This is getting repetitive isn’t it?
The theory is that long Covid has an autoimmune component as well as possibly being due to long-term damage to body tissues. But there are some reasons why this might not be the case.
The reason for thinking this is autoimmune is that most of the problems with severe Covid-19 are due to inflammation and the patient’s immune response to the infection. This is why immunosuppression with drugs like corticosteroids reduce the mortality from severe Covid-19. Many of the symptoms and signs of Covid-19, such as liver and kidney disease as well as encephalitis, occur in parts of the body where doctors have not “detected” any presence of the SARS CoV2. Clinicians and researches have looked for virus by PCR in these other places and not found it. The symptoms and signs in these other places are being caused by the over-reaction of the immune system in response to the virus within the lungs; the inflammation spreads around the body affecting these other sites… it is all due to widespread inflammation not direct viral infection. It is thought that long Covid is also a response to this immune triggered inflammation AFTER the virus has been cleared from the patient; the inflammation persists and causes ongoing symptoms. It’s a bit like a swollen ankle, the inflammation remains long after the trauma has gone and sticks around causing other problems.
On the other hand, there is no correlation between severity of Covid-19 and the development of long Covid; that is long Covid occurs equally frequently with mild, moderate or severe infection. That would provide support against a severe inflammatory cause of long Covid, as patients with mild Covid-19 don’t get the serve inflammatory response, but it could still be autoimmune! Many autoimmune diseases are due to the presence of antibodies produced during an acute illness that accidentally target normal host cells (known as autoantibodies). It’s therefore possible that long Covid is caused by something like these autoantibodies, but so far we just don’t know.
How is long Covid treated?
It may come as no surprise to know that since we don’t know the cause of long Covid we also don’t know how to specifically treat it. I say specifically because we can still treat the symptoms, but we have no wonder drug that turns off the disease process allowing patients to return to normal.
Some symptoms are more difficult to treat than others. For example, pain can be treated with over the counter medications such as Paracetamol or Ibuprofen, and breathlessness may respond to asthma inhalers, muscle weakness with physiotherapy and exercise regimes, gastrointestinal disturbances with dietary advice etc. Treatment gets more difficult though with things like insomnia where more specialist drugs such as melatonin may help. But when we get to the neurological problems such as cognitive impairment or psychological problems things get really tricky. These are very labour intensive and time consuming to treat using things such as cognitive behavioural therapy and may just not be practical based on the current under resourcing of these services.
It has been estimated that long Covid will cost the NHS £2.65 billion to manage but I think this is wishful thinking. It’s not the money that’s the “issue”, it’s the resources! We now have enormous waiting lists for non-Covid treatments (4.4 million), we have who knows how many people with undiagnosed illnesses who haven’t presented to their doctors during the pandemic (referrals from GPs were six million lower in 2020 than the year before), added to this we have a work force which is burnt out and we have chronic staffing shortages across the healthcare sector (my department has been short ¼ staffing for over 2 years because there is no one applying for the vacancies, but as “hidden pathology” infection specialists we might be considered non-essential and not first in line for resources!?). Do we really think this is just about finding some more money? Who is actually going to deliver the treatment of long-Covid?! Is this yet another role for “Consultant” or “Prescribing” physiotherapists, dietitians, pharmacists and nurses?
So, what do I think about long Covid?
I think long Covid exists… but the long and the short of it is that’s about the extent of what I think. After this there is a massive gap in my (our) knowledge:
…and that’s the problem.
Remember a year ago when the media was full of conflicting stories about Covid-19, where it came from, how to treat it, are we all going to die? All of that mayhem was based around a lack of knowledge. Lack of knowledge leads to fear and misinformation. We need to start filling in the knowledge gaps about long-Covid as quick as we can so that we can start managing it safely and effectively, otherwise the gap will be filled with misinformation and that has the potential to be much more damaging to the treatment of long-Covid in the long-term.
Perhaps the real elephant in the room is obesity; even the medical team in the Dispatches program were overweight and the patients bigger still! Being obese is a major risk factor for severe infection and suffering long Covid. Our nation is overweight and like other overweight nations we have fared far worse due to Covid-19 as a result (see graph from the New York Times below). This is not about having a go at people who are overweight but a fact; we must address the health of our nation and the answer is not just about taxing sugar, “Change for life”, “Couch to 5K” or “eating 5-a-day” campaigns. This needs something more drastic.
The NICE guideline states that:
“Symptoms after acute Covid-19 are highly variable and wide-ranging. The most commonly reported include (but are not limited to) the following:”
- Respiratory – breathlessness and cough
- Cardiovascular – chest tightness, chest pain and palpitations
- Neurological – cognitive impairment (‘brain fog’, loss of concentration or memory issues), headache, sleep disturbance, pins and needles, numbness, dizziness and delirium
- Gastrointestinal – abdominal pain, nausea, diarrhoea and reduced appetite
- Musculoskeletal – joint and muscle pains
- Psychological – depression and anxiety
- Ear, Nose and Throat (ENT) – tinnitus, earache, sore throat, dizziness, loss of taste or smell
- Dermatological – skin rashes, hair loss
- Generalised – fatigue, fever and pain
So essentially almost any symptoms can occur after Covid-19! In the small number of clinical studies looking at long Covid the most common symptoms are fatigue, cough, headache, loss of sense of smell or taste and muscle pain. But there should be a caveat here too and that is that those are usually the symptoms “asked about” in those studies and so any other symptoms could be missed, and the results become biased.
It is also difficult to identify which of the symptoms are due to some form of long-term disease, i.e. long Covid, and which are due to damage caused during the acute illness (e.g. breathlessness and cough following a severe lung infection) and which are due to the psychological trauma of being very sick and in a Critical Care Unit (e.g. cognitive impairment, sleep disturbance, depression and anxiety). All are valid symptoms but not necessarily due to the “virus” itself, but more the consequences of having had the virus.
How common is long Covid?
Long Covid appears to be common. The latest figures from the ONS suggest that 22.1% of patients still have symptoms at 5 weeks, and 9.8% still have symptoms at 12 weeks. That’s huge! In the UK we have had 4.26 million cases with 126,000 deaths. That means that there are 4.134 million Covid-19 survivors in the UK, which extrapolates to about 400,000 people who still had symptoms 12 weeks after acute Covid-19!
Long Covid is also more common in females, those aged 35-49 years and the obese. In particular long Covid is more common in the main working age groups, and therefore the socio-economic impact of long Covid-19, both on the individual as well as society, could be equally huge. And yet it has attracted little research so far. This seems short-sighted to me; the more we know about it the better we should be at managing it.
What is the cause of long Covid?
Guess what? No one agrees as no one knows!!!! This is getting repetitive isn’t it?
The theory is that long Covid has an autoimmune component as well as possibly being due to long-term damage to body tissues. But there are some reasons why this might not be the case.
The reason for thinking this is autoimmune is that most of the problems with severe Covid-19 are due to inflammation and the patient’s immune response to the infection. This is why immunosuppression with drugs like corticosteroids reduce the mortality from severe Covid-19. Many of the symptoms and signs of Covid-19, such as liver and kidney disease as well as encephalitis, occur in parts of the body where doctors have not “detected” any presence of the SARS CoV2. Clinicians and researches have looked for virus by PCR in these other places and not found it. The symptoms and signs in these other places are being caused by the over-reaction of the immune system in response to the virus within the lungs; the inflammation spreads around the body affecting these other sites… it is all due to widespread inflammation not direct viral infection. It is thought that long Covid is also a response to this immune triggered inflammation AFTER the virus has been cleared from the patient; the inflammation persists and causes ongoing symptoms. It’s a bit like a swollen ankle, the inflammation remains long after the trauma has gone and sticks around causing other problems.
On the other hand, there is no correlation between severity of Covid-19 and the development of long Covid; that is long Covid occurs equally frequently with mild, moderate or severe infection. That would provide support against a severe inflammatory cause of long Covid, as patients with mild Covid-19 don’t get the serve inflammatory response, but it could still be autoimmune! Many autoimmune diseases are due to the presence of antibodies produced during an acute illness that accidentally target normal host cells (known as autoantibodies). It’s therefore possible that long Covid is caused by something like these autoantibodies, but so far we just don’t know.
How is long Covid treated?
It may come as no surprise to know that since we don’t know the cause of long Covid we also don’t know how to specifically treat it. I say specifically because we can still treat the symptoms, but we have no wonder drug that turns off the disease process allowing patients to return to normal.
Some symptoms are more difficult to treat than others. For example, pain can be treated with over the counter medications such as Paracetamol or Ibuprofen, and breathlessness may respond to asthma inhalers, muscle weakness with physiotherapy and exercise regimes, gastrointestinal disturbances with dietary advice etc. Treatment gets more difficult though with things like insomnia where more specialist drugs such as melatonin may help. But when we get to the neurological problems such as cognitive impairment or psychological problems things get really tricky. These are very labour intensive and time consuming to treat using things such as cognitive behavioural therapy and may just not be practical based on the current under resourcing of these services.
It has been estimated that long Covid will cost the NHS £2.65 billion to manage but I think this is wishful thinking. It’s not the money that’s the “issue”, it’s the resources! We now have enormous waiting lists for non-Covid treatments (4.4 million), we have who knows how many people with undiagnosed illnesses who haven’t presented to their doctors during the pandemic (referrals from GPs were six million lower in 2020 than the year before), added to this we have a work force which is burnt out and we have chronic staffing shortages across the healthcare sector (my department has been short ¼ staffing for over 2 years because there is no one applying for the vacancies, but as “hidden pathology” infection specialists we might be considered non-essential and not first in line for resources!?). Do we really think this is just about finding some more money? Who is actually going to deliver the treatment of long-Covid?! Is this yet another role for “Consultant” or “Prescribing” physiotherapists, dietitians, pharmacists and nurses?
So, what do I think about long Covid?
I think long Covid exists… but the long and the short of it is that’s about the extent of what I think. After this there is a massive gap in my (our) knowledge:
- We don’t know the cause
- We don’t know how long it lasts
- We don’t know the symptoms
- We don’t know how to prevent it
- We don’t know how to treat it
- We don’t know if this only occurs after the first infection or whether it can occur after subsequent infections
- We just don’t know…
…and that’s the problem.
Remember a year ago when the media was full of conflicting stories about Covid-19, where it came from, how to treat it, are we all going to die? All of that mayhem was based around a lack of knowledge. Lack of knowledge leads to fear and misinformation. We need to start filling in the knowledge gaps about long-Covid as quick as we can so that we can start managing it safely and effectively, otherwise the gap will be filled with misinformation and that has the potential to be much more damaging to the treatment of long-Covid in the long-term.
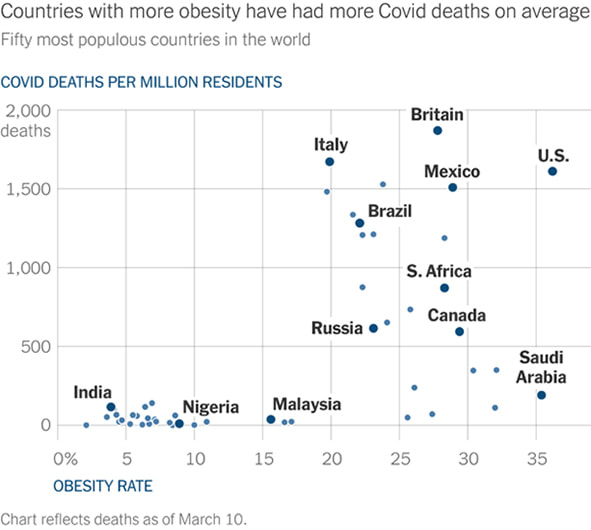
Perhaps the real elephant in the room is obesity; even the medical team in the Dispatches program were overweight and the patients bigger still! Being obese is a major risk factor for severe infection and suffering long Covid. Our nation is overweight and like other overweight nations we have fared far worse due to Covid-19 as a result (see graph from the New York Times below). This is not about having a go at people who are overweight but a fact; we must address the health of our nation and the answer is not just about taxing sugar, “Change for life”, “Couch to 5K” or “eating 5-a-day” campaigns. This needs something more drastic.
Click for larger image
Now I don’t profess to have the answer to this problem either. But obesity is a risk for so many medical problems not just severe Covid-19: heart disease, cancer, respiratory problems and many infections. And the problem is getting worse… perhaps the pandemic is the perfect opportunity to start to address this… Do you have any answers?
 RSS Feed
RSS Feed
