There seems to be huge amount of confusion about what tests are available for Covid-19. It doesn’t help that politicians and the media keep using the wrong terms and don’t understand what the different tests tell us. The squabbles seem to surround the numbers delivered rather than correct testing!
There are 3 main tests that are currently being discussed:
In order to understand the value of these tests it is important to understand the basic structure of a virus.
The structure of a virus
There are 3 main tests that are currently being discussed:
- Polymerase Chain Reaction (PCR) commonly referred to as a “molecular test”
- Antigen (Ag)
- Antibody (IgM and IgG)
In order to understand the value of these tests it is important to understand the basic structure of a virus.
The structure of a virus
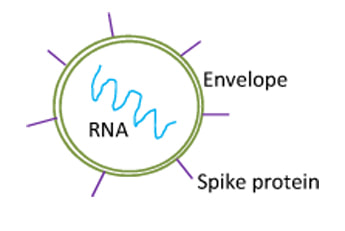
A virus essentially consists of an outer surface which encloses the rest of the virus. In the context of SARS Cov2 this is an outer fatty layer called the envelope (green). On the surface of the envelope are proteins, some of which are called “spike proteins” (purple) which give the virus it’s “crown” appearance and hence it’s classification as a coronavirus. It also makes a great graphic for the media… whereas bacillus bacteria are just boring rods! In the centre of the virus is the genetic material that encodes the production of new virus; in coronaviruses this is a large piece of single-stranded RNA (Ribonucleic Acid) shown in turquoise.
When a virus infects a cell the virus binds to the cell using the cell surface proteins and viral RNA is inserted into the cell. The cell then starts to use the virus’ genetic material, producing new virus. Once enough new virus has been produced the cell is usually killed and the new viruses are released to infect adjacent cells. The virus isn’t able to reproduce itself; it hijacks the cells reproductive mechanisms which then make more virus.
[As an aside, the fact that a virus isn’t able to reproduce outside of a cell means the virus cannot mutate outside of a cell; mutation in any organism only occurs during reproduction… no reproduction, no mutation, no antimicrobial resistance!]
Current Polymerase Chain Reaction (PCR) test – the test everyone is talking about!
The current Covid-19 test that everyone is talking about (everyone wants it, Boots the Chemist doesn’t sell it and no it is not available in the form of a home kit!) detects the genetic material of the virus, that is the RNA inside the virus.
PCR tests take small undetectable amounts of genetic material and then use enzymes to make more copies of the material until they reach levels that can be detected. PCR tests normally only detect DNA (Deoxyribonucleic Acid), so for SARS Cov2 there is an initial step called reverse transcription where the RNA is first converted to DNA before being amplified. This type of PCR is known as Reverse Transcriptase PCR or RT-PCR.
PCR tests are usually very specific (close to 100%). The test is targeted against genes that are only found in the target microorganism and so if the test is positive the identity of the microorganism is confirmed. PCR tests are also usually very sensitive, working by detecting very small amounts of genetic material and then amplifying them up. However, like many tests, PCRs are only as good as the sample being tested! In the context of SARS Cov2 it is very difficult to take a good nasopharyngeal sample; it is very uncomfortable to have a swab pushed to the very back of your nose (past where your finger can reach!!) and so often only the front of the nose is sampled. As a result the sensitivity of the Covid-19 PCR test only seems to be around 70%.
When a virus infects a cell the virus binds to the cell using the cell surface proteins and viral RNA is inserted into the cell. The cell then starts to use the virus’ genetic material, producing new virus. Once enough new virus has been produced the cell is usually killed and the new viruses are released to infect adjacent cells. The virus isn’t able to reproduce itself; it hijacks the cells reproductive mechanisms which then make more virus.
[As an aside, the fact that a virus isn’t able to reproduce outside of a cell means the virus cannot mutate outside of a cell; mutation in any organism only occurs during reproduction… no reproduction, no mutation, no antimicrobial resistance!]
Current Polymerase Chain Reaction (PCR) test – the test everyone is talking about!
The current Covid-19 test that everyone is talking about (everyone wants it, Boots the Chemist doesn’t sell it and no it is not available in the form of a home kit!) detects the genetic material of the virus, that is the RNA inside the virus.
PCR tests take small undetectable amounts of genetic material and then use enzymes to make more copies of the material until they reach levels that can be detected. PCR tests normally only detect DNA (Deoxyribonucleic Acid), so for SARS Cov2 there is an initial step called reverse transcription where the RNA is first converted to DNA before being amplified. This type of PCR is known as Reverse Transcriptase PCR or RT-PCR.
PCR tests are usually very specific (close to 100%). The test is targeted against genes that are only found in the target microorganism and so if the test is positive the identity of the microorganism is confirmed. PCR tests are also usually very sensitive, working by detecting very small amounts of genetic material and then amplifying them up. However, like many tests, PCRs are only as good as the sample being tested! In the context of SARS Cov2 it is very difficult to take a good nasopharyngeal sample; it is very uncomfortable to have a swab pushed to the very back of your nose (past where your finger can reach!!) and so often only the front of the nose is sampled. As a result the sensitivity of the Covid-19 PCR test only seems to be around 70%.
Don't forget to wash your hands!
This lack of sensitivity isn’t great but it is the best and only test we currently have available. This is why people like me are saying to colleagues if they have a patient who looks like they have Covid-19 clinically (e.g. cough, fever, hypoxia, high respiratory rate, bilateral chest signs and low lymphocytes) then the patient should be managed as Covid-19 irrespective of the PCR test result; Covid-19 is so common at the moment that there is no other realistic diagnosis for a patient with THIS combination of symptoms and signs.
Added to this, PCR tests do not tell you whether you have viable living infectious virus. They only tell you about the presence or absence of viral genetics in the sample. Even broken up bits of virus, meaning the virus is no longer able to infect anyone, will give a positive test; the test stays positive for a lot longer than infectious virus remains. This is important as many people seem to want to see a “negative PCR test” before deciding if a patient is non-infectious; in some patients the PCR can remain positive for up to 14 days even if there is no longer any infectious virus as determined by studies that have not found viable virus from day 7 onwards (that is why the isolation period is 7 days too).
Capacity of PCR testing
There has been a lot of discussion in the media, and lots of criticism from outside of Government, relating to problems around capacity of testing. The problem faced by laboratories isn’t one of lack of willingness, extended coffee breaks or inability, but rather infrastructure!
In order to do a PCR test for an infectious disease you need a number of key things:
Laboratory services have been quick to identify and put in place 1-3 above but they have no control over 4 and 5 and this is where the system has broken down. We have the platforms, the staff and the transport but we have struggled to get enough swabs to test patients and we have been unable to get enough reagents to perform the tests. This is often due to the suppliers being unable to cope with a massive surge in demand as well as importation problems as many of these items are produced by overseas companies.
It’s a basic supply and demand mismatch; the NHS is demanding the tests but the suppliers are unable to meet the demand. Therefore adding new eager “volunteer” laboratories will not solve the perceived “lack of capacity issues”. UK laboratories work to set national standards, a set of standard operating procedures (SOPs); this ensures the tests are standardised, valid, validated and accurate. Some new laboratories will perform well using these SOPs others might not; the NHS labs are closely regulated by UKAS (United Kingdom Accreditation Service) to ensure we do. Accurate valid tests are good tests; numerous inaccurate tests are not helpful. Anyhow, whichever lab processes the samples we’ll all still require more swabs and reagents!
Antigen tests
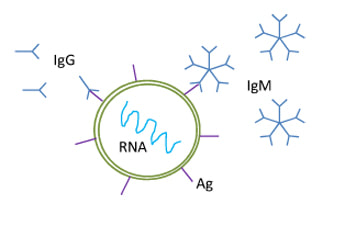
The politicians and media keep referring to antigen tests. Antigen tests detect fragments of virus or molecules, usually proteins, on the outer layer of a microorganism. These tests require laboratories to develop an antibody that “recognises” and binds to the antigen (Ag); the laboratory is essentially making a fake immune response it can then “find”. If the created antibody also contains a molecule, such as a coloured molecule, that can be detected, then the amount of molecule/colour produced will correspond to the amount of antibody and hence the amount of bound antigen.
Antigen tests can be very sensitive but unless there is a very good match between the lab’s antibody and the antigen they can be prone to false positive results. False positives occur because the antibody is reacting to a different but “similar” antigen in the sample; it’s like the lab’s antibody is colour blind and cannot distinguish between red and orange. In the context of Covid-19 this false positive antigen could be an antigen from one of the other similar 4 seasonal coronaviruses which cause the common cold in the UK every year.
Added to this, PCR tests do not tell you whether you have viable living infectious virus. They only tell you about the presence or absence of viral genetics in the sample. Even broken up bits of virus, meaning the virus is no longer able to infect anyone, will give a positive test; the test stays positive for a lot longer than infectious virus remains. This is important as many people seem to want to see a “negative PCR test” before deciding if a patient is non-infectious; in some patients the PCR can remain positive for up to 14 days even if there is no longer any infectious virus as determined by studies that have not found viable virus from day 7 onwards (that is why the isolation period is 7 days too).
Capacity of PCR testing
There has been a lot of discussion in the media, and lots of criticism from outside of Government, relating to problems around capacity of testing. The problem faced by laboratories isn’t one of lack of willingness, extended coffee breaks or inability, but rather infrastructure!
In order to do a PCR test for an infectious disease you need a number of key things:
- A machine that does the test (called a platform)
- A highly skilled workforce trained to run the platform
- Transport to the laboratory; invariably transportation to a distant testing laboratory affects turnaround times
- The sampling kits, in this case swabs in viral transport medium (that keeps the sample viable)
- The chemicals that the platform uses to do the test (reagents)
Laboratory services have been quick to identify and put in place 1-3 above but they have no control over 4 and 5 and this is where the system has broken down. We have the platforms, the staff and the transport but we have struggled to get enough swabs to test patients and we have been unable to get enough reagents to perform the tests. This is often due to the suppliers being unable to cope with a massive surge in demand as well as importation problems as many of these items are produced by overseas companies.
It’s a basic supply and demand mismatch; the NHS is demanding the tests but the suppliers are unable to meet the demand. Therefore adding new eager “volunteer” laboratories will not solve the perceived “lack of capacity issues”. UK laboratories work to set national standards, a set of standard operating procedures (SOPs); this ensures the tests are standardised, valid, validated and accurate. Some new laboratories will perform well using these SOPs others might not; the NHS labs are closely regulated by UKAS (United Kingdom Accreditation Service) to ensure we do. Accurate valid tests are good tests; numerous inaccurate tests are not helpful. Anyhow, whichever lab processes the samples we’ll all still require more swabs and reagents!
Antigen tests
The politicians and media keep referring to antigen tests. Antigen tests detect fragments of virus or molecules, usually proteins, on the outer layer of a microorganism. These tests require laboratories to develop an antibody that “recognises” and binds to the antigen (Ag); the laboratory is essentially making a fake immune response it can then “find”. If the created antibody also contains a molecule, such as a coloured molecule, that can be detected, then the amount of molecule/colour produced will correspond to the amount of antibody and hence the amount of bound antigen.
Antigen tests can be very sensitive but unless there is a very good match between the lab’s antibody and the antigen they can be prone to false positive results. False positives occur because the antibody is reacting to a different but “similar” antigen in the sample; it’s like the lab’s antibody is colour blind and cannot distinguish between red and orange. In the context of Covid-19 this false positive antigen could be an antigen from one of the other similar 4 seasonal coronaviruses which cause the common cold in the UK every year.

Click for larger image
The interest in antigen tests for Covid-19 lies with “pregnancy style” test kits which can give a rapid (within 15 minutes) result at a patient’s bedside. If they can be produced with very good sensitivity and specificity and not cross react with other viruses they will be very useful providing a rapid way of deciding whether a patient should be managed in a Covid-19 or non-Covid-19 area or it could be used in nursing homes to help segregate infected from non-infected residents.
Do Covid-19 Ag tests exist?
Currently there “ten CE-marked rapid SARS-CoV-2 antigen detection tests*, meaning they conform with the relevant EU legislation, Directive 98/79/EC on IVDs” (European Centre for Disease Prevention and Control, 1st April 2020) available commercially. However, *the manufacturer themselves has to specify device performance characteristics and self-declare conformity with the safety and performance requirements! Official EU “moderators” have identified several devices with fraudulent documentation, incomplete technical files or unsubstantiated claims; they have also found the kits to be less accurate and less sensitive than laboratory-performed diagnostic tests. Currently in the UK they are not available to purchase, some countries have even prohibited them.
As for the consumer testing market, it’s awash with claims about different kits but the Medicines and Healthcare products Regulatory Agency (MHRA) state there are no CE marked tests for home use and it is illegal to supply such products.
Antibody tests
These are the tests we healthcare professionals want! These are the tests that tell us whether our patients or colleagues have HAD Covid-19 in the past. We normally look for 2 types of antibody, IgM and IgG.
Antibodies (these are our body’s natural immune response, not the lab generated ones in antigen tests) help the immune system recognise the virus or virally infected cells and get rid of them, sometimes killing the cell the virus is in as well! Ultimately this is the way the body deals with the infection, but it can lead to damage to the body if too many cells are killed off.
IgM tests
IgM is the first antibody produced by the patient’s immune system in response to an infection. It usually takes about a week for IgM to first be produced. IgM is a pentamer (5 components joined together) which is relatively non-specific about what antigen (Ag) it binds to; its shape helps it to adapt to fit or attach to various antigens. It has to be relatively non-specific as the body is only just reacting to the infection so it needs to make sure the antibody can recognise “variations of intruder” and react to the infection (e.g. above Covid-19 had red Ag and “common cold” had orange Ag).
Do Covid-19 Ag tests exist?
Currently there “ten CE-marked rapid SARS-CoV-2 antigen detection tests*, meaning they conform with the relevant EU legislation, Directive 98/79/EC on IVDs” (European Centre for Disease Prevention and Control, 1st April 2020) available commercially. However, *the manufacturer themselves has to specify device performance characteristics and self-declare conformity with the safety and performance requirements! Official EU “moderators” have identified several devices with fraudulent documentation, incomplete technical files or unsubstantiated claims; they have also found the kits to be less accurate and less sensitive than laboratory-performed diagnostic tests. Currently in the UK they are not available to purchase, some countries have even prohibited them.
As for the consumer testing market, it’s awash with claims about different kits but the Medicines and Healthcare products Regulatory Agency (MHRA) state there are no CE marked tests for home use and it is illegal to supply such products.
Antibody tests
These are the tests we healthcare professionals want! These are the tests that tell us whether our patients or colleagues have HAD Covid-19 in the past. We normally look for 2 types of antibody, IgM and IgG.
Antibodies (these are our body’s natural immune response, not the lab generated ones in antigen tests) help the immune system recognise the virus or virally infected cells and get rid of them, sometimes killing the cell the virus is in as well! Ultimately this is the way the body deals with the infection, but it can lead to damage to the body if too many cells are killed off.
IgM tests
IgM is the first antibody produced by the patient’s immune system in response to an infection. It usually takes about a week for IgM to first be produced. IgM is a pentamer (5 components joined together) which is relatively non-specific about what antigen (Ag) it binds to; its shape helps it to adapt to fit or attach to various antigens. It has to be relatively non-specific as the body is only just reacting to the infection so it needs to make sure the antibody can recognise “variations of intruder” and react to the infection (e.g. above Covid-19 had red Ag and “common cold” had orange Ag).
IgM tests can be used to diagnose acute infection as IgM is made during the initial period of infection, however they can be prone to false positives as the IgM can “overreact” to all sorts of non-specific antigens in the patient’s sample. In reality an IgM test will be of little additional value above and beyond the current PCR tests, so concentrating efforts to develop this test is not so useful clinically. It may help diagnose the 30% of false negatives with PCR due to the poor sampling, but better sampling would be better still. Remember: False negatives - if a patient looks like they have Covid-19, then they have Covid-19!
IgG tests
As the body becomes more “experienced” at dealing with an infection it starts to produce more precise antibody called IgG, usually 2-3 weeks after the infection begins. IgG is a monomer (single component) which is directed against the specific viral antigens. It is much more “sticky” for the antigens than IgM and is a more effective “flag” for the immune system to see and therefore get rid of the infection. However 2-3 weeks is too long to wait for Covid-19 as non-symptomatic isolators are out of isolation in 14 days. Added to this it is also important to recognise that IgG tests could cross react with the 4 UK seasonal coronaviruses, which would again give false positives.
In the longer term, the cells that produce IgG become part of the immune systems memory so that next time the immune system comes into contact with the microorganism the cells capable of producing IgG can be rapidly reproduced in order to prevent infection. This is the principle of long term immunity and forms the basis for the effectiveness of vaccinations. The value of IgG testing lies in detecting the presence of IgG to SARS Cov2 in the greater population, indicating “herd immunity”. Herd immunity works as it stops the virus being able to spread; the virus infects someone but their immune system kicks in, which destroys the virus before it takes hold or has the chance to transmit to another person, and even if it does transmit that new person is also probably immune and ready to fight it off, stopping transmission.
So remember, IgG tests CANNOT be used to diagnose acute infections as they are not positive during the first 2-3 weeks of an illness and often only become positive when the infection starts to resolve. They can however be used to see who has had an infection in the past and who is therefore immune to future infections.
Unfortunately currently there are no IgM or IgG tests available… but the NHS and PHE are working on it…
Testing healthcare workers
The current PCR testing of healthcare workers who are self-isolating due to living with a Covid-19 contact is slightly politically driven. If the healthcare worker tests negative on day 3 or 5 etc. of self-isolation they should still be required to isolate for 14 days to ensure they do not develop symptoms on day 4, or 6 etc. The NEED for those healthcare workers however may draw “early tested negatives” back to work when theoretically they could still test positive! It’s a difficult balance between risk of infection and risk of no healthcare workers! If healthcare workers test positive they require 7 days to become “clear” of infection; remember their PCR test many remain positive after this due to fragments of DNA not active virus.
Why test healthcare workers then?
IgG testing of healthcare workers would be helpful. If someone who has “had” Covid-19 (maybe weeks before) but was “asymptomatic”, is now being isolated due to a family contact then an IgG test will detect this immunity. IgG will tell us who amongst us has had the infection already and is therefore fit for work even if there is someone else at home who has symptoms consistent with Covid-19; this IgG test will really help us manage the healthcare workforce including doctors, nurses, carers etc. However this test is also not yet available!
What tests do I want?
Okay, so for those of us working in the NHS we have been told that the Easter bank holidays are to be treated like any other working day. It looks like I won’t be getting that Thornton’s Special Toffee Easter Egg after all… (Added to the fact that Thornton’s website states “Due to high demand, we have temporarily paused taking new orders!” ECIC is trying!!)
So if I can’t have an Easter egg what Covid-19 diagnostic tests do I want and why?
This is what I want, what I really, really want:
Oh, but only the PCR is available at present and that’s in short supply… sounds like strong bread flour and toilet roll to me! Have a good Easter and if you’re one of us working then I hope it isn’t too bad for you.
Stay sane!
IgG tests
As the body becomes more “experienced” at dealing with an infection it starts to produce more precise antibody called IgG, usually 2-3 weeks after the infection begins. IgG is a monomer (single component) which is directed against the specific viral antigens. It is much more “sticky” for the antigens than IgM and is a more effective “flag” for the immune system to see and therefore get rid of the infection. However 2-3 weeks is too long to wait for Covid-19 as non-symptomatic isolators are out of isolation in 14 days. Added to this it is also important to recognise that IgG tests could cross react with the 4 UK seasonal coronaviruses, which would again give false positives.
In the longer term, the cells that produce IgG become part of the immune systems memory so that next time the immune system comes into contact with the microorganism the cells capable of producing IgG can be rapidly reproduced in order to prevent infection. This is the principle of long term immunity and forms the basis for the effectiveness of vaccinations. The value of IgG testing lies in detecting the presence of IgG to SARS Cov2 in the greater population, indicating “herd immunity”. Herd immunity works as it stops the virus being able to spread; the virus infects someone but their immune system kicks in, which destroys the virus before it takes hold or has the chance to transmit to another person, and even if it does transmit that new person is also probably immune and ready to fight it off, stopping transmission.
So remember, IgG tests CANNOT be used to diagnose acute infections as they are not positive during the first 2-3 weeks of an illness and often only become positive when the infection starts to resolve. They can however be used to see who has had an infection in the past and who is therefore immune to future infections.
Unfortunately currently there are no IgM or IgG tests available… but the NHS and PHE are working on it…
Testing healthcare workers
The current PCR testing of healthcare workers who are self-isolating due to living with a Covid-19 contact is slightly politically driven. If the healthcare worker tests negative on day 3 or 5 etc. of self-isolation they should still be required to isolate for 14 days to ensure they do not develop symptoms on day 4, or 6 etc. The NEED for those healthcare workers however may draw “early tested negatives” back to work when theoretically they could still test positive! It’s a difficult balance between risk of infection and risk of no healthcare workers! If healthcare workers test positive they require 7 days to become “clear” of infection; remember their PCR test many remain positive after this due to fragments of DNA not active virus.
Why test healthcare workers then?
IgG testing of healthcare workers would be helpful. If someone who has “had” Covid-19 (maybe weeks before) but was “asymptomatic”, is now being isolated due to a family contact then an IgG test will detect this immunity. IgG will tell us who amongst us has had the infection already and is therefore fit for work even if there is someone else at home who has symptoms consistent with Covid-19; this IgG test will really help us manage the healthcare workforce including doctors, nurses, carers etc. However this test is also not yet available!
What tests do I want?
Okay, so for those of us working in the NHS we have been told that the Easter bank holidays are to be treated like any other working day. It looks like I won’t be getting that Thornton’s Special Toffee Easter Egg after all… (Added to the fact that Thornton’s website states “Due to high demand, we have temporarily paused taking new orders!” ECIC is trying!!)
So if I can’t have an Easter egg what Covid-19 diagnostic tests do I want and why?
This is what I want, what I really, really want:
- Rapid Ag test – an accurate “pregnancy style” antigen test to tell me who has Covid-19 both in hospital and in nursing homes
- IgG antibody test – to tell me who are the healthcare workers who have had Covid-19 and who are then able to be at work
- PCR - mixed in with a normal respiratory PCR panel (a multiplex PCR) for detecting all of the common respiratory pathogens for the next time SARS Cov2 comes back into the population and I want to spot it quickly and stop it spreading again…
Oh, but only the PCR is available at present and that’s in short supply… sounds like strong bread flour and toilet roll to me! Have a good Easter and if you’re one of us working then I hope it isn’t too bad for you.
Stay sane!
 RSS Feed
RSS Feed
