The patient was a young woman with the most severe headache she had ever had. She was normally fit and well. Her headache was so bad that she kept a towel over her eyes because the light made it worse. She was noted to have a fever and so a provisional diagnosis of meningitis was made.
Whilst taking her history the doctor discovered that she had returned from the USA at the weekend where she had been visiting family. In particular she had been staying in New York. The doctor consulted “Dr Google” and found mention of a cause of meningitis called West Nile Virus. They called the duty Microbiologist to ask for additional tests on the CSF sent earlier to the lab.
“Stone the Crows” thought the Microbiologist after he got over the slight irritation from the lack of initial travel history documented on the request card. He had to admit though that he was pleased that the doctor had taken the trouble to look into this patient’s story in more detail and then do something with the new knowledge they had acquired.
Whilst taking her history the doctor discovered that she had returned from the USA at the weekend where she had been visiting family. In particular she had been staying in New York. The doctor consulted “Dr Google” and found mention of a cause of meningitis called West Nile Virus. They called the duty Microbiologist to ask for additional tests on the CSF sent earlier to the lab.
“Stone the Crows” thought the Microbiologist after he got over the slight irritation from the lack of initial travel history documented on the request card. He had to admit though that he was pleased that the doctor had taken the trouble to look into this patient’s story in more detail and then do something with the new knowledge they had acquired.
Further tests were arranged but the patient was treated empirically for the more likely bacterial meningitis with IV Ceftriaxone whilst awaiting the lab results.
So what is West Nile Virus, and what has the West Nile got to do with New York?
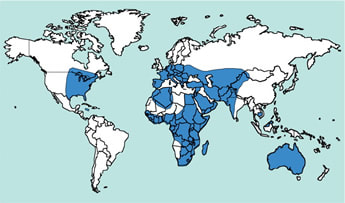
West Nile Virus was first discovered in 1937 in the West Nile region of Uganda in Africa… hence its name. It is also found in Europe and neighbouring countries including Romania, Italy, Hungary, Austria, Russia and Israel, all the way across to China and the USA and down to Australia, as well as large parts of Africa.
So what is West Nile Virus, and what has the West Nile got to do with New York?
West Nile Virus was first discovered in 1937 in the West Nile region of Uganda in Africa… hence its name. It is also found in Europe and neighbouring countries including Romania, Italy, Hungary, Austria, Russia and Israel, all the way across to China and the USA and down to Australia, as well as large parts of Africa.
West Nile Virus is a Flavivirus in the same family as Japanese encephalitis and yellow fever. It is transmitted through the bite of Culex mosquitoes which usually bite between dusk and dawn. The main hosts for West Nile Virus are birds. Some birds such as chickens become highly viraemic without becoming unwell whereas others such as crows become viraemic and die. In either case mosquitoes that “feed” off viraemic birds also become infected which can then infect humans. Human-to-human transmission has occurred through blood transfusion, organ transplantation, during pregnancy and also possibly through breast feeding, but these are all very rare.
West Nile Virus became more widely known after an outbreak in New York in the USA between August and September 1999. During this time there were 59 cases of West Nile Virus infection including 37 cases of encephalitis; 7 patients died. This was the first time West Nile Virus had been documented in the USA. At the same time large numbers of birds were dying in the New York City area. Necropsy of these specimens eventually identified West Nile Virus in these birds and the link between birds and humans was made.
How does infection with West Nile Virus present?
The incubation period for infection with West Nile Virus is normally 2-6 days, but it can be as high as 21 days in immunosuppressed patients.
Infection with West Nile Virus can present in a number of different ways:
West Nile fever is a self-limiting problem but the neuroinvasive disease is a serious infection associated with long-term sequelae and a relatively high mortality.
West Nile meningitis is clinically indistinguishable from other forms of viral meningitis. The patient presents with fever, headache, photophobia and neck stiffness. CSF analysis shows a raised lymphocyte count, a normal glucose and a normal or only slightly raised protein. The mortality from West Nile meningitis is approximately 2% yet up to 40% of patients who have had West Nile meningitis experience long-term neurological symptoms such as fatigue, weakness, depression and chronic pain.
West Nile encephalitis presents with seizures, altered mental state, focal neurological signs and occasionally movement disorders. CSF can be normal or show a similar pattern to meningitis. The prognosis for encephalitis is much worse with 12% mortality. In addition up to 70% of those who survive experience long-term neurological problems.
West Nile flaccid paralysis, sometimes known as “West Nile poliomyelitis” because it mimics poliomyelitis, is caused by damage to the anterior horn cells of the spinal cord. This leads to acute muscle weakness and possible progression to respiratory failure and death if not given supportive ventilation.
How is West Nile Virus infection diagnosed?
Like all infections the clinical history is the clue to making a diagnosis of West Nile Virus, including the all-important travel history. At present we do not have West Nile Virus in the UK and so for someone to present with West Nile Virus infection they would have to have acquired it abroad. The main places where West Nile Virus is found include Southern Europe (Greece, Italy and Spain), USA, Canada, the Middle East, Australia, Russia, Southern Asia and parts of Africa. In fact it has the potential to occur in any place which has both the Culex mosquitos that transmit it and the birds that are the amplifying hosts (and this would include the UK if the virus was introduced here, “Stone the Crows!”).
In endemic countries there is often a preceding alert from Public Health Departments when West Nile Virus is thought to be in an area, often recognised by a very high mortality rate in birds of the crow family (corvidae); if corvids start to die they are tested for West Nile and this generates the alert to healthcare professionals.
The laboratory diagnosis of West Nile Virus is based on either finding evidence of the virus using PCR or evidence of the patient’s immune response by antibody tests.
If the patient presents early enough (i.e. within a few days of onset of symptoms) then PCR can be done on CSF and urine to look for the virus. Unfortunately most patients do not present this quickly, or the diagnosis is not considered within this time frame, and therefore the PCR is often negative. So a negative PCR does not rule out the diagnosis of West Nile Virus infection, it is only of value if it is positive in which case it confirms the diagnosis.
The mainstay of diagnosis is the detection of antibodies against West Nile Virus, both IgM and IgG. Patients with West Nile Virus start to produce IgM within about a week of infection. This can be detected in serum - confirming infection, and CSF - confirming neuroinvasive disease. If the IgM is negative and West Nile Virus is still strongly suspected then a convalescent serum sample should be taken 2-3 weeks later to look for the presence of IgG. A fourfold rise in IgG confirms recent infection.
Remember that IgG is also evidence of past infection and so it is important that the amount of IgG between the acute and convalescent samples has increased fourfold otherwise it is likely to represent either past infection with West Nile Virus, infection with a different cross-reacting flavivirus or immunisation against a different flavivirus (e.g. Japanese encephalitis or yellow fever).
How is West Nile Virus infection treated?
There is no specific treatment for West Nile Virus; treatment is supportive. Interferon, Ribavirin and Immunoglobulin have all been tried in cases outside of controlled trials and at best they don’t work and at worst they may actually cause harm. So proceed with care!
How can West Nile Virus infection be prevented?
There are no specific infection control precautions for West Nile Virus infection; standard universal precautions are adequate. The virus is not usually found in the body fluids of patients with infection.
In terms of prevention of West Nile Virus infections in the community this involves: control of the mosquito vector, surveillance of disease in birds and prevention of bites in humans.
Mosquitoes breed in still water and therefore a critical aspect of mosquito control is to eliminate all standing water to which the mosquito can get access. This can be open water storage tanks, old tyres, buckets, open bottles or jars, anything that holds water.
The next aspect for preventing infections is to look for unexpected deaths in birds from the crow family. If this is noted they should be tested for West Nile Virus and alerts given to local healthcare professionals to be on the lookout for infections so they can be diagnosed quickly and supportive care given promptly.
The final aspect of prevention is for people to avoid being bitten by Culex mosquitoes. This involves covering up between dusk and dawn with long trousers and sleeves, using insect repellents and sleeping in air-conditioned rooms under mosquito nets.
So our patient’s CSF showed viral meningitis but the tests for West Nile Virus were negative. The CSF did however contain Enterovirus RNA so it turned out the patient had the most common cause of viral meningitis we see in the UK. Her IV Ceftriaxone for bacterial meningitis was stopped and she made a quick recovery. But, But, But…West Nile Virus was still an important part of the patient’s differential diagnosis even if it wasn’t the cause this time… maybe next time though…
West Nile Virus became more widely known after an outbreak in New York in the USA between August and September 1999. During this time there were 59 cases of West Nile Virus infection including 37 cases of encephalitis; 7 patients died. This was the first time West Nile Virus had been documented in the USA. At the same time large numbers of birds were dying in the New York City area. Necropsy of these specimens eventually identified West Nile Virus in these birds and the link between birds and humans was made.
How does infection with West Nile Virus present?
The incubation period for infection with West Nile Virus is normally 2-6 days, but it can be as high as 21 days in immunosuppressed patients.
Infection with West Nile Virus can present in a number of different ways:
- Asymptomatic (70-80%)
- West Nile fever (20-30%) - fever, headache, myalgia, arthralgia and gastrointestinal symptoms, there is also often a transient maculopapular rash
- Neuroinvasive disease (<1%) – meningitis, encephalitis or flaccid paralysis
- Very rare cases of myocarditis and cardiac arrhythmias, rhabdomyolysis, optic neuritis, uveitis, chorioretinitis, orchitis, hepatitis and pancreatitis.
West Nile fever is a self-limiting problem but the neuroinvasive disease is a serious infection associated with long-term sequelae and a relatively high mortality.
West Nile meningitis is clinically indistinguishable from other forms of viral meningitis. The patient presents with fever, headache, photophobia and neck stiffness. CSF analysis shows a raised lymphocyte count, a normal glucose and a normal or only slightly raised protein. The mortality from West Nile meningitis is approximately 2% yet up to 40% of patients who have had West Nile meningitis experience long-term neurological symptoms such as fatigue, weakness, depression and chronic pain.
West Nile encephalitis presents with seizures, altered mental state, focal neurological signs and occasionally movement disorders. CSF can be normal or show a similar pattern to meningitis. The prognosis for encephalitis is much worse with 12% mortality. In addition up to 70% of those who survive experience long-term neurological problems.
West Nile flaccid paralysis, sometimes known as “West Nile poliomyelitis” because it mimics poliomyelitis, is caused by damage to the anterior horn cells of the spinal cord. This leads to acute muscle weakness and possible progression to respiratory failure and death if not given supportive ventilation.
How is West Nile Virus infection diagnosed?
Like all infections the clinical history is the clue to making a diagnosis of West Nile Virus, including the all-important travel history. At present we do not have West Nile Virus in the UK and so for someone to present with West Nile Virus infection they would have to have acquired it abroad. The main places where West Nile Virus is found include Southern Europe (Greece, Italy and Spain), USA, Canada, the Middle East, Australia, Russia, Southern Asia and parts of Africa. In fact it has the potential to occur in any place which has both the Culex mosquitos that transmit it and the birds that are the amplifying hosts (and this would include the UK if the virus was introduced here, “Stone the Crows!”).
In endemic countries there is often a preceding alert from Public Health Departments when West Nile Virus is thought to be in an area, often recognised by a very high mortality rate in birds of the crow family (corvidae); if corvids start to die they are tested for West Nile and this generates the alert to healthcare professionals.
The laboratory diagnosis of West Nile Virus is based on either finding evidence of the virus using PCR or evidence of the patient’s immune response by antibody tests.
If the patient presents early enough (i.e. within a few days of onset of symptoms) then PCR can be done on CSF and urine to look for the virus. Unfortunately most patients do not present this quickly, or the diagnosis is not considered within this time frame, and therefore the PCR is often negative. So a negative PCR does not rule out the diagnosis of West Nile Virus infection, it is only of value if it is positive in which case it confirms the diagnosis.
The mainstay of diagnosis is the detection of antibodies against West Nile Virus, both IgM and IgG. Patients with West Nile Virus start to produce IgM within about a week of infection. This can be detected in serum - confirming infection, and CSF - confirming neuroinvasive disease. If the IgM is negative and West Nile Virus is still strongly suspected then a convalescent serum sample should be taken 2-3 weeks later to look for the presence of IgG. A fourfold rise in IgG confirms recent infection.
Remember that IgG is also evidence of past infection and so it is important that the amount of IgG between the acute and convalescent samples has increased fourfold otherwise it is likely to represent either past infection with West Nile Virus, infection with a different cross-reacting flavivirus or immunisation against a different flavivirus (e.g. Japanese encephalitis or yellow fever).
How is West Nile Virus infection treated?
There is no specific treatment for West Nile Virus; treatment is supportive. Interferon, Ribavirin and Immunoglobulin have all been tried in cases outside of controlled trials and at best they don’t work and at worst they may actually cause harm. So proceed with care!
How can West Nile Virus infection be prevented?
There are no specific infection control precautions for West Nile Virus infection; standard universal precautions are adequate. The virus is not usually found in the body fluids of patients with infection.
In terms of prevention of West Nile Virus infections in the community this involves: control of the mosquito vector, surveillance of disease in birds and prevention of bites in humans.
Mosquitoes breed in still water and therefore a critical aspect of mosquito control is to eliminate all standing water to which the mosquito can get access. This can be open water storage tanks, old tyres, buckets, open bottles or jars, anything that holds water.
The next aspect for preventing infections is to look for unexpected deaths in birds from the crow family. If this is noted they should be tested for West Nile Virus and alerts given to local healthcare professionals to be on the lookout for infections so they can be diagnosed quickly and supportive care given promptly.
The final aspect of prevention is for people to avoid being bitten by Culex mosquitoes. This involves covering up between dusk and dawn with long trousers and sleeves, using insect repellents and sleeping in air-conditioned rooms under mosquito nets.
So our patient’s CSF showed viral meningitis but the tests for West Nile Virus were negative. The CSF did however contain Enterovirus RNA so it turned out the patient had the most common cause of viral meningitis we see in the UK. Her IV Ceftriaxone for bacterial meningitis was stopped and she made a quick recovery. But, But, But…West Nile Virus was still an important part of the patient’s differential diagnosis even if it wasn’t the cause this time… maybe next time though…
 RSS Feed
RSS Feed
