“Happy birthday to us, happy birthday to us, happy birthday dear Bug Blog, happy birthday to ussss…”
The Bug Blog is 5 years old! You may not realise it but we have been doing this together for 5 years. In that time we have written over 190 blogs on various microbiology related subjects as diverse as Proteus mirabilis (which Penny thinks smells like chocolate!), necrotising fasciitis and even Poldark’s Putrid Throat. It can be quite a challenge to find the time to write a blog every week but we strive to keep it up (on average we have managed about 40 per year). What makes it worthwhile is all of you out there taking the trouble to read what we have to say. So thank you for staying with us and reading all of our microbiological rambles…
The Bug Blog is 5 years old! You may not realise it but we have been doing this together for 5 years. In that time we have written over 190 blogs on various microbiology related subjects as diverse as Proteus mirabilis (which Penny thinks smells like chocolate!), necrotising fasciitis and even Poldark’s Putrid Throat. It can be quite a challenge to find the time to write a blog every week but we strive to keep it up (on average we have managed about 40 per year). What makes it worthwhile is all of you out there taking the trouble to read what we have to say. So thank you for staying with us and reading all of our microbiological rambles…

One of the great things about Microbiology is that no matter how long you have been studying it there is always the potential for something new to come along. So this week the subject is something that I had never heard of before and had to do some reading about when it cropped up in a patient (as always I’ve changed the case to protect the patient’s confidentiality).
The Microbiology Registrar was busy working through the blood culture list deciding what to ring out when they came across a new bacterium for them.
“What do you know about Actinotignum spp.” they asked their Consultant.
“Nothing, you made it up” replied the Consultant thinking this was just part of their normal daily banter and a way to stop him singing.
“No, there really is a blood culture which apparently has this bacterium in it from one of the urology wards, …honest!” replied the Registrar.
The Consultant checked the result for themselves and sure enough it looked genuine.
“Never heard of it. Probably a MaldiTOF thing and a load of rubbish. Why don’t you look it up and tell me what you find out” said the Consultant thinking this would be a good “learning experience” for the Registrar. The Registrar groaned and tutted lots…but went off to start the hunt for the “unknown”.
So what did the Registrar find out?
What are the Actinotignum species?
The Actinotignum spp. were only discovered 20 years ago in 1997 but are related to the Actinomycetes, a group of bacteria often described as weakly acid fast because they have some mycolic acid in their cell wall a bit like Mycobacteria spp. There are three different bacteria in the group: A. schaalii which is the most common and A. urinale and A. sanguinis. A. schaalii is name after a German Microbiologist, Klaus Schaal, who did lots of research on the Actinomycetes and is still a Professor of Microbiology at the University of Bonn. The other two bacteria are named because they are found in urine and blood… like their names suggest which is helpful for memory recall but not quite as cool as having a bacterium named after you I guess…
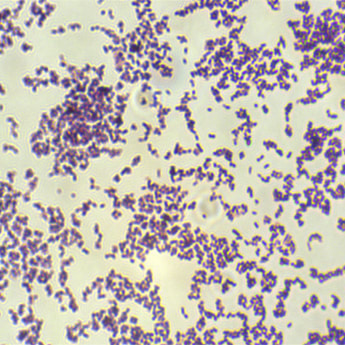
The Actinotignum spp. are small non-motile Gram-positive bacilli. They do not produce spores and are not acid fast. In fact they are pretty weedy. They are facultative anaerobes (fussy to grow) they require at least 48 hours of culture on enriched blood agar in 5% CO2 or an anaerobic incubator; they require the extra CO2. Remember that an anaerobic incubator is usually 15% CO2 to partially replace the oxygen. Actinotignum spp. are also very unreactive in various biochemical tests which is probably why the old fashioned identification methods of APIs couldn’t identify them… the bacteria didn’t really do anything and so gave a blank profile in the test.
For those of you who don’t remember, let me enlighten you about the fun and games of the random number generator of the APIs. They were a strip of biochemical reactions which were incubated overnight with the bacterium you wanted to identify and then each reaction was scored to generate a number sequence. The number sequence was put in a database and a bacterial name popped out…. In my experience the name was often not what was expected or even feasible much of the time (i.e. a Gram-negative bacterium went in but a Gram-positive name popped out!) often the Biomedical Scientist had to keep fiddling the results in order to get a remotely sensible answer… oh those were the days before MaldiTOF or whole genome sequencing rubbish… (Joking! I don’t miss APIs at all.)
So we have a pretty unreactive organism in terms of biochemical analysis, so is there anything about its colonial morphology that gives a clue to its identification? In a nutshell… no there isn’t. At 48 hours of culture on enriched blood agar in CO2 all you have are tiny grey weakly beta-haemolytic colonies (< 1mm diameter).
The Microbiology Registrar was busy working through the blood culture list deciding what to ring out when they came across a new bacterium for them.
“What do you know about Actinotignum spp.” they asked their Consultant.
“Nothing, you made it up” replied the Consultant thinking this was just part of their normal daily banter and a way to stop him singing.
“No, there really is a blood culture which apparently has this bacterium in it from one of the urology wards, …honest!” replied the Registrar.
The Consultant checked the result for themselves and sure enough it looked genuine.
“Never heard of it. Probably a MaldiTOF thing and a load of rubbish. Why don’t you look it up and tell me what you find out” said the Consultant thinking this would be a good “learning experience” for the Registrar. The Registrar groaned and tutted lots…but went off to start the hunt for the “unknown”.
So what did the Registrar find out?
What are the Actinotignum species?
The Actinotignum spp. were only discovered 20 years ago in 1997 but are related to the Actinomycetes, a group of bacteria often described as weakly acid fast because they have some mycolic acid in their cell wall a bit like Mycobacteria spp. There are three different bacteria in the group: A. schaalii which is the most common and A. urinale and A. sanguinis. A. schaalii is name after a German Microbiologist, Klaus Schaal, who did lots of research on the Actinomycetes and is still a Professor of Microbiology at the University of Bonn. The other two bacteria are named because they are found in urine and blood… like their names suggest which is helpful for memory recall but not quite as cool as having a bacterium named after you I guess…
The Actinotignum spp. are small non-motile Gram-positive bacilli. They do not produce spores and are not acid fast. In fact they are pretty weedy. They are facultative anaerobes (fussy to grow) they require at least 48 hours of culture on enriched blood agar in 5% CO2 or an anaerobic incubator; they require the extra CO2. Remember that an anaerobic incubator is usually 15% CO2 to partially replace the oxygen. Actinotignum spp. are also very unreactive in various biochemical tests which is probably why the old fashioned identification methods of APIs couldn’t identify them… the bacteria didn’t really do anything and so gave a blank profile in the test.
For those of you who don’t remember, let me enlighten you about the fun and games of the random number generator of the APIs. They were a strip of biochemical reactions which were incubated overnight with the bacterium you wanted to identify and then each reaction was scored to generate a number sequence. The number sequence was put in a database and a bacterial name popped out…. In my experience the name was often not what was expected or even feasible much of the time (i.e. a Gram-negative bacterium went in but a Gram-positive name popped out!) often the Biomedical Scientist had to keep fiddling the results in order to get a remotely sensible answer… oh those were the days before MaldiTOF or whole genome sequencing rubbish… (Joking! I don’t miss APIs at all.)
So we have a pretty unreactive organism in terms of biochemical analysis, so is there anything about its colonial morphology that gives a clue to its identification? In a nutshell… no there isn’t. At 48 hours of culture on enriched blood agar in CO2 all you have are tiny grey weakly beta-haemolytic colonies (< 1mm diameter).

So it’s unreactive and looks pathetic, so do we really need to worry about it?
Clinical significance of Actinotignum spp.
The only bacterium of the species that is clinically relevant is A. schaalii, yep so those names urinale and sanguinis might mean “urine” and a “blood-red colour” but clinically they don’t match up! As of 2016 there had been 172 case reports of infections caused by A. schaalii. Most were UTIs but some bacteraemias and other infections had also been reported:
I do think we need to be a little careful when using data from such a small group of case reports as they may not actually represent the exact rates of infection with this bacterium. It may be that in most situations where this bacterium is isolated, laboratories will not bother to try and give it a name, or they may just report it generically as either a Gram-positive bacillus or “coryneform bacterium” of uncertain significance, or they may not report it at all thinking it is probably a skin contaminant. The only time a laboratory or Microbiologists is like to pursue the “name” is when it is isolated from a sterile site (e.g. in a blood culture) or when someone is convinced it is more significant (e.g. a urine from a patient with recurrent pyuria not responding to conventional treatments). Or when the Registrar asks the Consultant what it is and they have never heard of it before! So cases of A. schaalii infection may actually be under reported.
The most common clinical features in A. schaalii infections are: patients aged > 60 years old who have an underlying urinary tract abnormality e.g. bladder cancer, urinary catheterisation, prostate problems or other obstructed urinary tracts. Even bacteraemias with A. schaalii almost always appear to be related to urinary tract problems. This isn’t actually that surprising when you consider where A. schaalii normally lives…
Where is A. schaalii normal flora?
Studies on both healthy and hospitalised volunteers have shown that A. schaalii can be found in 22% of adult urine samples and 33% of urine samples from under 4 year olds. All of the people in these studies with A. schaalii in their urine were asymptomatic. It has also been found in 33% of vaginal samples from asymptomatic women. Again the number of people in these studies was small but the studies do suggest that A. schaalii might be part of the normal flora of the urinary tract.
This is also supported by studies of the bacterium itself which have shown that it has genes that produce proteins involved in binding to urothelial cells allowing it to both colonise the urinary tract as well as cause UTIs, in much the same way that bacteria such as E. coli and Klebsiella spp. do. However unlike E. coli and Klebsiella spp. which are normal flora of the bowel and transfer into the urinary tract to cause infections, the studies have failed to find A. schaalii in the bowel. This suggests that A. schaalii is genuinely urinary tract normal flora and not an accidental invader of the urinary tract from the bowel.
However the fact that 20-30% of asymptomatic people seem to carry A. schaalii in their urinary tract raises the possibility of over reporting the significance of A. schaalii as being the cause of UTI in the case reports. It is entirely possible that the case reports might be mistaking colonisation for infection, i.e. the urine sample grows the bacterium but the bacterium is not the cause of the patient’s symptoms.
It’s a tricky dilemma, how do you distinguish colonisation and infection? The studies showed that by treating the bacterium it goes away along with the patient’s symptoms and therefore they draw the conclusion that A. schaalii is causative. Although this is not 100% proof, I’m inclined to believe them as it is more probable that the bacterium was the cause rather than an innocent bystander or coloniser. If the bacterium were a coloniser then when you eradicate that coloniser the symptoms usually do not disappear, in fact the multiple “treatments” tend to just select out more resistant bacteria who have survived the onslaught of antimicrobials.
How do you diagnose A. schaalii infection?
In general A. schaalii UTI is going to be under recognised as most urine samples are incubated for only 24 hours, on chromogenic agar that doesn’t include blood and which is incubated in air… none of which is going to allow A. schaalii to be isolated. Note: This is the National Standard Operating Procedure (SOP) in the UK so pretty much every laboratory in the UK is going to fail to isolate this bacterium. Not only that, if they did by some chance manage to grow the bacterium they might reject the colonies as not being typical urinary tract pathogens or fail to identify them if they don’t have MaldiTOF available.
To make matters worse the sample may not actually get sent to the laboratory because A. schaalii doesn’t produce nitrate reductase and therefore doesn’t give a bacterial nitrite reaction on a urine dipstick test! The urine dipstick is the first point of care test used in the Public Health England primary care guideline to determine if there is a UTI!! This might lead the doctors to exclude a UTI even though there are white blood cells present (see how to interpret a urine result blog!).
So the only way you would diagnose A. schaalii infection is to consider it in the first place. The UK SOP does kind of allow for this, in that if you have a patient with recurrent pyuria (white blood cells) in urine then you can culture on blood agar for 48 hours in CO2, but it’s not very clear how you might pick up on these patients amongst the hundreds of thousands of urines per year being processed, especially as most forms don’t have any clinical information on them let alone specific details to help identify the need for specific testing.
So if you do find someone has an infection with A. schaalii how do you treat them?
One of the problems with treating A. schaalii UTIs is that the bacterium is resistant to Trimethoprim (and Co-trimoxazole) as well as often being resistant to Fosfomycin and Mecillinam, all of which are commonly used to treat UTIs as they are part of the 1st line treatments in the Public Health England primary care guideline for the treatment of UTIs. The fluoroquinolones are also not very effective with complete resistance to Ciprofloxacin and high levels of resistance to Levofloxacin and Moxifloxacin. A. schaalii is sensitive to Nitrofurantoin which would be suitable for a simple UTI but not pyelonephritis or bacteraemia, or many frail renally defunct old folk due to toxicity (see previous blog).
Of the antibiotics commonly used to treat UTIs the most reliable drugs are Amoxicillin, cephalosporins and aminoglycosides, such as Gentamicin. Antibiotics that are not usually considered to be urinary tract antibiotics but are also active include Doxycycline, glycopeptides, such as Teicoplanin and Vancomycin, Linezolid and the other beta-lactams (except Mecillinam).
Personally I would use Amoxicillin or Doxycycline orally to treat simple UTIs with A. schaalii and IV Amoxicillin or IV Gentamicin for bacteraemias occurring secondary to UTIs. However there have been some treatment failures with the 1 week treatment courses, therefore it might be prudent to consider a 2 week course, but there is no definite evidence for this.
“Ha, told you it was real!” said the Registrar as she finished presenting all the information.
“Yes, yes” The Consultant had to concede… The Registrar had found out loads of information about Actinotignum spp., including the excellent review article in the references below. She also found out that the patient did have an abnormal urinary tract, had symptoms suggestive of a UTI, and had failed treatment with Trimethoprim, Fosfomycin and Ciprofloxacin for their “recurrent UTI” before being admitted now unwell (none of which was in the clinical details section of the request form!)
The patient was successfully treated with IV Amoxicillin and the Microbiology Consultant learnt something new… “All-in-all a good day’s work”, said the Consultant.
The Registrar raised her eyebrow… “All due to the hard work of your Registrar!” she said sarcastically as she left the room in search of a celebratory chocolate biscuit and just in time as her Consultant had started to sing again!!
“Happy birthday to us, happy birthday to us, happy blogdaaayyyy” … okay, okay, I’ll stop singing now….
So there you have it, the Bug Blog is 5 years old and still turning up new stuff…
P.S. Thank you Registrars!
Reference
Actinotignum schaalii (formerly Actinobaculum schaalii: a newly recognized pathogen – review of the literature. Lotte, R, Lotte L, Ruimy R. Clin Microbiol Infect 2016; 22: 28-36
Clinical significance of Actinotignum spp.
The only bacterium of the species that is clinically relevant is A. schaalii, yep so those names urinale and sanguinis might mean “urine” and a “blood-red colour” but clinically they don’t match up! As of 2016 there had been 172 case reports of infections caused by A. schaalii. Most were UTIs but some bacteraemias and other infections had also been reported:
- UTI = 121 (70%)
- Bacteraemia = 33 (19%)
- Abscess = 12 (7%)
- Cellulitis = 2 (1.5%)
- Disciitis (inflammation or infection of the intervertebral discs) = 2 (1.5%)
- Endocarditis 1 (0.5%)
- Fournier’s gangrene (a type of necrotising fasciitis) = 1 (0.5%)
I do think we need to be a little careful when using data from such a small group of case reports as they may not actually represent the exact rates of infection with this bacterium. It may be that in most situations where this bacterium is isolated, laboratories will not bother to try and give it a name, or they may just report it generically as either a Gram-positive bacillus or “coryneform bacterium” of uncertain significance, or they may not report it at all thinking it is probably a skin contaminant. The only time a laboratory or Microbiologists is like to pursue the “name” is when it is isolated from a sterile site (e.g. in a blood culture) or when someone is convinced it is more significant (e.g. a urine from a patient with recurrent pyuria not responding to conventional treatments). Or when the Registrar asks the Consultant what it is and they have never heard of it before! So cases of A. schaalii infection may actually be under reported.
The most common clinical features in A. schaalii infections are: patients aged > 60 years old who have an underlying urinary tract abnormality e.g. bladder cancer, urinary catheterisation, prostate problems or other obstructed urinary tracts. Even bacteraemias with A. schaalii almost always appear to be related to urinary tract problems. This isn’t actually that surprising when you consider where A. schaalii normally lives…
Where is A. schaalii normal flora?
Studies on both healthy and hospitalised volunteers have shown that A. schaalii can be found in 22% of adult urine samples and 33% of urine samples from under 4 year olds. All of the people in these studies with A. schaalii in their urine were asymptomatic. It has also been found in 33% of vaginal samples from asymptomatic women. Again the number of people in these studies was small but the studies do suggest that A. schaalii might be part of the normal flora of the urinary tract.
This is also supported by studies of the bacterium itself which have shown that it has genes that produce proteins involved in binding to urothelial cells allowing it to both colonise the urinary tract as well as cause UTIs, in much the same way that bacteria such as E. coli and Klebsiella spp. do. However unlike E. coli and Klebsiella spp. which are normal flora of the bowel and transfer into the urinary tract to cause infections, the studies have failed to find A. schaalii in the bowel. This suggests that A. schaalii is genuinely urinary tract normal flora and not an accidental invader of the urinary tract from the bowel.
However the fact that 20-30% of asymptomatic people seem to carry A. schaalii in their urinary tract raises the possibility of over reporting the significance of A. schaalii as being the cause of UTI in the case reports. It is entirely possible that the case reports might be mistaking colonisation for infection, i.e. the urine sample grows the bacterium but the bacterium is not the cause of the patient’s symptoms.
It’s a tricky dilemma, how do you distinguish colonisation and infection? The studies showed that by treating the bacterium it goes away along with the patient’s symptoms and therefore they draw the conclusion that A. schaalii is causative. Although this is not 100% proof, I’m inclined to believe them as it is more probable that the bacterium was the cause rather than an innocent bystander or coloniser. If the bacterium were a coloniser then when you eradicate that coloniser the symptoms usually do not disappear, in fact the multiple “treatments” tend to just select out more resistant bacteria who have survived the onslaught of antimicrobials.
How do you diagnose A. schaalii infection?
In general A. schaalii UTI is going to be under recognised as most urine samples are incubated for only 24 hours, on chromogenic agar that doesn’t include blood and which is incubated in air… none of which is going to allow A. schaalii to be isolated. Note: This is the National Standard Operating Procedure (SOP) in the UK so pretty much every laboratory in the UK is going to fail to isolate this bacterium. Not only that, if they did by some chance manage to grow the bacterium they might reject the colonies as not being typical urinary tract pathogens or fail to identify them if they don’t have MaldiTOF available.
To make matters worse the sample may not actually get sent to the laboratory because A. schaalii doesn’t produce nitrate reductase and therefore doesn’t give a bacterial nitrite reaction on a urine dipstick test! The urine dipstick is the first point of care test used in the Public Health England primary care guideline to determine if there is a UTI!! This might lead the doctors to exclude a UTI even though there are white blood cells present (see how to interpret a urine result blog!).
So the only way you would diagnose A. schaalii infection is to consider it in the first place. The UK SOP does kind of allow for this, in that if you have a patient with recurrent pyuria (white blood cells) in urine then you can culture on blood agar for 48 hours in CO2, but it’s not very clear how you might pick up on these patients amongst the hundreds of thousands of urines per year being processed, especially as most forms don’t have any clinical information on them let alone specific details to help identify the need for specific testing.
So if you do find someone has an infection with A. schaalii how do you treat them?
One of the problems with treating A. schaalii UTIs is that the bacterium is resistant to Trimethoprim (and Co-trimoxazole) as well as often being resistant to Fosfomycin and Mecillinam, all of which are commonly used to treat UTIs as they are part of the 1st line treatments in the Public Health England primary care guideline for the treatment of UTIs. The fluoroquinolones are also not very effective with complete resistance to Ciprofloxacin and high levels of resistance to Levofloxacin and Moxifloxacin. A. schaalii is sensitive to Nitrofurantoin which would be suitable for a simple UTI but not pyelonephritis or bacteraemia, or many frail renally defunct old folk due to toxicity (see previous blog).
Of the antibiotics commonly used to treat UTIs the most reliable drugs are Amoxicillin, cephalosporins and aminoglycosides, such as Gentamicin. Antibiotics that are not usually considered to be urinary tract antibiotics but are also active include Doxycycline, glycopeptides, such as Teicoplanin and Vancomycin, Linezolid and the other beta-lactams (except Mecillinam).
Personally I would use Amoxicillin or Doxycycline orally to treat simple UTIs with A. schaalii and IV Amoxicillin or IV Gentamicin for bacteraemias occurring secondary to UTIs. However there have been some treatment failures with the 1 week treatment courses, therefore it might be prudent to consider a 2 week course, but there is no definite evidence for this.
“Ha, told you it was real!” said the Registrar as she finished presenting all the information.
“Yes, yes” The Consultant had to concede… The Registrar had found out loads of information about Actinotignum spp., including the excellent review article in the references below. She also found out that the patient did have an abnormal urinary tract, had symptoms suggestive of a UTI, and had failed treatment with Trimethoprim, Fosfomycin and Ciprofloxacin for their “recurrent UTI” before being admitted now unwell (none of which was in the clinical details section of the request form!)
The patient was successfully treated with IV Amoxicillin and the Microbiology Consultant learnt something new… “All-in-all a good day’s work”, said the Consultant.
The Registrar raised her eyebrow… “All due to the hard work of your Registrar!” she said sarcastically as she left the room in search of a celebratory chocolate biscuit and just in time as her Consultant had started to sing again!!
“Happy birthday to us, happy birthday to us, happy blogdaaayyyy” … okay, okay, I’ll stop singing now….
So there you have it, the Bug Blog is 5 years old and still turning up new stuff…
P.S. Thank you Registrars!
Reference
Actinotignum schaalii (formerly Actinobaculum schaalii: a newly recognized pathogen – review of the literature. Lotte, R, Lotte L, Ruimy R. Clin Microbiol Infect 2016; 22: 28-36
 RSS Feed
RSS Feed
