The patient was in his mid-twenties and was clearly terrified. He was escorted in to the Emergency Department by his mother who quickly explained to the triage Nurse what she thought was going on.
“He’s had a stroke his face is drooping and he can’t speak properly!” she cried.
The Nurse looked at the patient and it was clear that his face was drooping on the left hand side.
“When did this start?” the Nurse asked in a calm voice.
“I woke up like this this morning”. He said struggling but he understood the question and had a recognisable speech pattern, but he was dribbling. “It’s awful” he continued. The patient looked like he was going to run screaming from the department.
“He’s had a stroke his face is drooping and he can’t speak properly!” she cried.
The Nurse looked at the patient and it was clear that his face was drooping on the left hand side.
“When did this start?” the Nurse asked in a calm voice.
“I woke up like this this morning”. He said struggling but he understood the question and had a recognisable speech pattern, but he was dribbling. “It’s awful” he continued. The patient looked like he was going to run screaming from the department.
She asked him “can you smile” … while she observed, “OK that looks tricky for you… Arms… can you lift and hold up both arms?” … “Yes… good…” said the Nurse.
FAST is the acronym being promoted to the UK public in order to recognise a person having a stroke (Facial drooping, Arm weakness, Speech difficulties and Time to call the emergency services)
“Okay, I’m sure it’s not a stroke. I think it’s something called a Bell’s palsy. But let’s get you seen by the Doctor and go from there” the Nurse advised.
What is a Bell’s palsy?
Bell’s palsy is paralysis of the facial muscles as a result of a problem with the facial nerve. It is named after Sir Charles Bell who first described the anatomy of the facial nerve back in the early 1800s.
The facial nerve is the 7th cranial nerve (nerves arising directly from the brain). It arises from the pons of the brain, goes through the internal auditory meatus to the side of the face, where it passes under the parotid gland in the cheek.
The facial nerve provides a nerve supply to:
A Bell’s palsy therefore affects the nerve distribution of the facial nerve which is most notable as paralysis of the facial muscles.
How does a Bell’s palsy present?
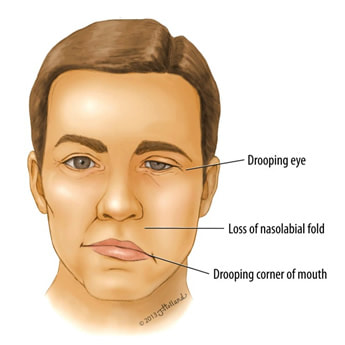
Paralysis of the facial muscles is sudden in onset getting worse over a few hours, and typically only affects one side of the face. The corner of the mouth droops and the patient may start to dribble saliva. The eyebrow sags and the patient is unable to close their eye properly. Patients often don’t notice but they also lose the nasolabial fold (the place where the cheek muscles dip in to meet the base of the nose).
Other symptoms can include a reduction in ability to produce tears, an increased sensitivity to noise and a loss of ability to taste food and drink.
Weakness usually presents within a day but can continue to get worse over 3 weeks, if they continue to worsen beyond this point an alternative cause of the facial palsy should be sought. Also Bell’s palsy normally shows at least some recovery by 4 months.
FAST is the acronym being promoted to the UK public in order to recognise a person having a stroke (Facial drooping, Arm weakness, Speech difficulties and Time to call the emergency services)
“Okay, I’m sure it’s not a stroke. I think it’s something called a Bell’s palsy. But let’s get you seen by the Doctor and go from there” the Nurse advised.
What is a Bell’s palsy?
Bell’s palsy is paralysis of the facial muscles as a result of a problem with the facial nerve. It is named after Sir Charles Bell who first described the anatomy of the facial nerve back in the early 1800s.
The facial nerve is the 7th cranial nerve (nerves arising directly from the brain). It arises from the pons of the brain, goes through the internal auditory meatus to the side of the face, where it passes under the parotid gland in the cheek.
The facial nerve provides a nerve supply to:
- Facial muscles
- Lacrimal, submandibular and sublingual salivary glands
- Taste on the front two thirds of the tongue
- Sensation from the external auditory canal and the pinna of the ear
A Bell’s palsy therefore affects the nerve distribution of the facial nerve which is most notable as paralysis of the facial muscles.
How does a Bell’s palsy present?
Paralysis of the facial muscles is sudden in onset getting worse over a few hours, and typically only affects one side of the face. The corner of the mouth droops and the patient may start to dribble saliva. The eyebrow sags and the patient is unable to close their eye properly. Patients often don’t notice but they also lose the nasolabial fold (the place where the cheek muscles dip in to meet the base of the nose).
Other symptoms can include a reduction in ability to produce tears, an increased sensitivity to noise and a loss of ability to taste food and drink.
Weakness usually presents within a day but can continue to get worse over 3 weeks, if they continue to worsen beyond this point an alternative cause of the facial palsy should be sought. Also Bell’s palsy normally shows at least some recovery by 4 months.

Click for larger image

Remember: branches of the facial nerve follow the 5 fingers
What is going on…environmental plastic pollution, elephants and veterinary stuff, this week neurology! What the heck has this got to do with microbiology!?! … keep reading…
What causes a Bell’s palsy?
When Bell’s palsy was first described (and even up until I was a junior doctor… which was not the early 1800s thank you very much!) there was little known about the cause. It was described as an idiopathic paralysis of the facial nerve; this is the posh way of saying the cause was unknown but I suspect lots of doctors don’t want to admit they don’t know something, so they use terms like idiopathic!
We now suspect that most Bell’s palsies are caused by reactivation of Herpes Simplex Virus (HSV); the virus that causes labial cold sores. Studies have found HSV DNA in facial nerve fluid and tissue as well as muscle in about 75% of adult patients (but only about 5% in children). Varicella Zoster Virus (VZV) has been found in another 6-7% of both adults and children. These viruses cause inflammation and demyelination of the facial nerve. See a microbiological cause!
HSV and VZV are plausible causes as both sit latent in nerve ganglia and reactivate in the distribution of those nerves. HSV causes cold sores and VZV causes shingles. Both of these conditions are associated with changes in the distribution of sensory nerves (the characteristic blistering of the skin), whereas in Bells’ palsy the reactivation is in a motor nerve hence weakness occurs rather than skin changes. One exception to this is when VZV reactivates a bit higher up in the facial nerve distribution to involve the sensory nerve supply to the auditory canal in which case blisters occur inside the ear (known as Ramsay-Hunt syndrome).
Less common causes of Bell’s palsy include:
NB Strictly speaking Lyme disease and Ramsay-Hunt syndrome are specific diagnoses in their own right, but as they are both important and relatively common causes of facial nerve palsy I have included them above.
How is Bell’s palsy diagnosed?
Bell’s palsy is a clinical diagnosis; there is no specific laboratory test, the diagnosis is made in the presence of a good history and clinical signs. The most important aspect of the diagnosis is to make sure there is no other underlying problem such as a tumour pressing on the nerve which might account for the symptoms and signs. This is primarily done by ensuring no other cranial nerves are affected and that onset is acute (over a day or so). Another clue is that if there was a preceding twitch or spasm in the muscle in the days before paralysis occurred, this may indicate something is pressing on the nerve and therefore not a Bell’s palsy. Retrospectively recovery should also begin within four months.
If there is any doubt about the diagnosis then it is wise to arrange a CT or MRI scan of the head to look for other lesions.
The only Microbiology test routinely performed for Bell’s palsy is Lyme serology. This is because of all the potential causes, Lyme disease has specific treatment. The normal treatment is PO Doxycycline 100mg BD for 21 days in adults OR Amoxicillin 1g TDS for 21 days in children. Doxycycline is more effective than Amoxicillin, with a lower relapse rate, but Doxycycline is currently contraindicated in children, see previous blog. If the initial Lyme serology is negative but Lyme disease is strongly suspected (e.g. known tick bite) then it is worth repeating the serology after 4-6 weeks as it can take time for the antibodies, which the test looks for, to develop.
How is Bell’s palsy treated?
The mainstay of treatment for Bell’s palsy is early steroids given for 1 week. Ideally these should be started within 3 days of the onset of symptoms. They are often still given even if the patient presents later than this but they are less effective.
Many experts now also give 1 week of empirical Aciclovir or Valaciclovir to patients with Bell’s palsy to treat HSV and VSV as these are likely to be the cause in over 80%. The adult dose of Aciclovir is 800mg 5 times per day OR Valaciclovir is 1g TDS.
It is also important to take steps to protect the patient’s eye as when the eyelids don’t close it leaves the eye prone to damage from drying or trauma. Artificial tears in the form of eye drops are useful, as is a patch or protective goggles.
What is the prognosis for Bell’s palsy?
More than 85% of patients show some improvement within 3 weeks of symptoms appearing. More than 70% make a full recovery, 13% have a slight residual weakness but in 16% the weakness is more pronounced. Early steroids and antivirals increase the rate of full recovery to 94%. Recurrent episodes can occur in 5-10% of both adults and children but more than 2 episodes are very unusual.
So the young patient did indeed have a facial nerve palsy. His mother was eventually reassured that this was not a stroke. He was started on steroids and Valaciclovir and within three weeks had started to notice a bit of improvement. He did eventually make a full recovery, although his mother complained about her “nerves” for quite a while after…
What causes a Bell’s palsy?
When Bell’s palsy was first described (and even up until I was a junior doctor… which was not the early 1800s thank you very much!) there was little known about the cause. It was described as an idiopathic paralysis of the facial nerve; this is the posh way of saying the cause was unknown but I suspect lots of doctors don’t want to admit they don’t know something, so they use terms like idiopathic!
We now suspect that most Bell’s palsies are caused by reactivation of Herpes Simplex Virus (HSV); the virus that causes labial cold sores. Studies have found HSV DNA in facial nerve fluid and tissue as well as muscle in about 75% of adult patients (but only about 5% in children). Varicella Zoster Virus (VZV) has been found in another 6-7% of both adults and children. These viruses cause inflammation and demyelination of the facial nerve. See a microbiological cause!
HSV and VZV are plausible causes as both sit latent in nerve ganglia and reactivate in the distribution of those nerves. HSV causes cold sores and VZV causes shingles. Both of these conditions are associated with changes in the distribution of sensory nerves (the characteristic blistering of the skin), whereas in Bells’ palsy the reactivation is in a motor nerve hence weakness occurs rather than skin changes. One exception to this is when VZV reactivates a bit higher up in the facial nerve distribution to involve the sensory nerve supply to the auditory canal in which case blisters occur inside the ear (known as Ramsay-Hunt syndrome).
Less common causes of Bell’s palsy include:
- Lyme disease (Borrelia burgdorferi) - the most common cause of facial palsy in children, over 50% in some studies, as well as one of the few causes of bilateral facial nerve palsy
- Cytomegalovirus (CMV) – another herpes virus
- Epstein-Barr virus (EBV) – yet another herpes virus
- Adenovirus
- Rubella virus
- Mumps virus – can also cause facial nerve problems as it causes inflammation and swelling of the parotid gland which then presses on the facial nerve underneath
- Influenza B virus
- Coxsackie virus
NB Strictly speaking Lyme disease and Ramsay-Hunt syndrome are specific diagnoses in their own right, but as they are both important and relatively common causes of facial nerve palsy I have included them above.
How is Bell’s palsy diagnosed?
Bell’s palsy is a clinical diagnosis; there is no specific laboratory test, the diagnosis is made in the presence of a good history and clinical signs. The most important aspect of the diagnosis is to make sure there is no other underlying problem such as a tumour pressing on the nerve which might account for the symptoms and signs. This is primarily done by ensuring no other cranial nerves are affected and that onset is acute (over a day or so). Another clue is that if there was a preceding twitch or spasm in the muscle in the days before paralysis occurred, this may indicate something is pressing on the nerve and therefore not a Bell’s palsy. Retrospectively recovery should also begin within four months.
If there is any doubt about the diagnosis then it is wise to arrange a CT or MRI scan of the head to look for other lesions.
The only Microbiology test routinely performed for Bell’s palsy is Lyme serology. This is because of all the potential causes, Lyme disease has specific treatment. The normal treatment is PO Doxycycline 100mg BD for 21 days in adults OR Amoxicillin 1g TDS for 21 days in children. Doxycycline is more effective than Amoxicillin, with a lower relapse rate, but Doxycycline is currently contraindicated in children, see previous blog. If the initial Lyme serology is negative but Lyme disease is strongly suspected (e.g. known tick bite) then it is worth repeating the serology after 4-6 weeks as it can take time for the antibodies, which the test looks for, to develop.
How is Bell’s palsy treated?
The mainstay of treatment for Bell’s palsy is early steroids given for 1 week. Ideally these should be started within 3 days of the onset of symptoms. They are often still given even if the patient presents later than this but they are less effective.
Many experts now also give 1 week of empirical Aciclovir or Valaciclovir to patients with Bell’s palsy to treat HSV and VSV as these are likely to be the cause in over 80%. The adult dose of Aciclovir is 800mg 5 times per day OR Valaciclovir is 1g TDS.
It is also important to take steps to protect the patient’s eye as when the eyelids don’t close it leaves the eye prone to damage from drying or trauma. Artificial tears in the form of eye drops are useful, as is a patch or protective goggles.
What is the prognosis for Bell’s palsy?
More than 85% of patients show some improvement within 3 weeks of symptoms appearing. More than 70% make a full recovery, 13% have a slight residual weakness but in 16% the weakness is more pronounced. Early steroids and antivirals increase the rate of full recovery to 94%. Recurrent episodes can occur in 5-10% of both adults and children but more than 2 episodes are very unusual.
So the young patient did indeed have a facial nerve palsy. His mother was eventually reassured that this was not a stroke. He was started on steroids and Valaciclovir and within three weeks had started to notice a bit of improvement. He did eventually make a full recovery, although his mother complained about her “nerves” for quite a while after…
 RSS Feed
RSS Feed
