There is a change coming to how you will see laboratory culture results reported, but will you know what it means?
Within the UK, as well as most of the rest of Europe, laboratories follow a standard procedure for testing whether bacteria are likely to respond to treatment with different antibiotics. You see this on reports where the laboratory says a bacterium is susceptible (or sensitive) to an antibiotic which they mark with an “S” or resistant to an antibiotic which they mark with an “R”.
But did you notice that sometimes the laboratory puts an “I” for intermediate? And if you did, did you know what intermediate means?
Within the UK, as well as most of the rest of Europe, laboratories follow a standard procedure for testing whether bacteria are likely to respond to treatment with different antibiotics. You see this on reports where the laboratory says a bacterium is susceptible (or sensitive) to an antibiotic which they mark with an “S” or resistant to an antibiotic which they mark with an “R”.
But did you notice that sometimes the laboratory puts an “I” for intermediate? And if you did, did you know what intermediate means?

But Ref, what the heck does intermediate mean?!
Well, if not it doesn’t matter anymore because it’s changing!
A bacterium was designated as of intermediate susceptibility if it was inhibited by an antibiotic in the laboratory at a concentration “between” susceptible and resistant (“I” could therefore be “In the middle”). For example, susceptible might be a concentration < 2mg/L and resistant might be a concentration >8mg/L; in this case intermediate would mean a concentration of 2-8mg/L. BUT let’s be frank, this still doesn’t tell anyone how to interpret the result!!!
I suspect that most people thought the “I” stood for “Ignore it” and they just chose a different antibiotic, and when I was a junior doctor, I suspect I did the same thing. To add to the confusion, intermediate has two potential interpretations:
Having two different interpretations of intermediate is really unhelpful, which also makes it a pretty useless term in my opinion and “encourages” most people to Ignore it!
So, what…why tell us the lab test result is rubbish?
Well, Microbiology laboratories in the UK use an antibiotic susceptibility method set out by EUCAST (European Committee on Antimicrobial Susceptibility Testing). This is a huge part of what a microbiology laboratory “does”, and the method is updated every year with new values that define the results of susceptibility testing. YAWN!! It is one of those massive headaches laboratories have to undergo every year to make sure they adopt the new changes to the EUCAST method… it’s a bit of a chore really, lots of “subtle dullness” and paperwork etc.
However, something new and exciting is coming! Yes, these little things excite microbiologists… [Maybe “exciting” should also be a banned word along with interesting…] OK, OK, it is inappropriate to use exciting to describe changes to EUCAST reporting… but EUCAST are finally doing away with the intermediate susceptibility reporting… thank goodness!
You are still going to see susceptible and resistant, but the third type of report is going to be “susceptible at increased exposure”. Really!!! That’s not doing away with it, surely that’s just “tweaking” and semantics!!! Unfortunately, this doesn’t lend itself to an easy single letter for reporting, but locally we are going with S*, so that the isolate still looks susceptible.
Susceptible at increased exposure means that the bacterium is susceptible, but that an increased dose of antibiotic is needed; an increased dose can mean larger antibiotic doses and/or more frequent doses.
I do think this is better! No honest I do!!! It’s important to remember that nothing in medicine (and microbiology) is 100% accurate, and even though the laboratory might say a bacterium is susceptible the patient may not respond, and likewise the bacterium might be reported as resistant, but the patient gets better. This is because there are multiple factors in addition to laboratory testing that affect whether treatment is successful or not, including:
So, it’s important to interpret “susceptible at increased exposure” results as a guide to what antibiotics should treat a specific patient, rather than a guarantee that the treatment will work.
Different antibiotics have different ways of increasing the dose to correspond to an S* result. The table below shows the most important of these (assuming normal renal function, liver function and body mass index). For example, the normal dose of Amoxicillin is 1g TDS BUT the higher dose is 2g six times-a-day, for Temocillin the normal dose is 2g BD BUT the higher dose is 2g TDS, and for Ciprofloxacin the normal PO dose is 500mg BD BUT the higher dose is 750mg BD.
A bacterium was designated as of intermediate susceptibility if it was inhibited by an antibiotic in the laboratory at a concentration “between” susceptible and resistant (“I” could therefore be “In the middle”). For example, susceptible might be a concentration < 2mg/L and resistant might be a concentration >8mg/L; in this case intermediate would mean a concentration of 2-8mg/L. BUT let’s be frank, this still doesn’t tell anyone how to interpret the result!!!
I suspect that most people thought the “I” stood for “Ignore it” and they just chose a different antibiotic, and when I was a junior doctor, I suspect I did the same thing. To add to the confusion, intermediate has two potential interpretations:
- The isolate might be susceptible if the patient has higher than normal levels of antibiotic at the site of infection, for example the antibiotic concentrates in a particular location such as fluoroquinolones do in urine
- The isolate may respond to the antibiotic, but response is unpredictable based on laboratory testing
Having two different interpretations of intermediate is really unhelpful, which also makes it a pretty useless term in my opinion and “encourages” most people to Ignore it!
So, what…why tell us the lab test result is rubbish?
Well, Microbiology laboratories in the UK use an antibiotic susceptibility method set out by EUCAST (European Committee on Antimicrobial Susceptibility Testing). This is a huge part of what a microbiology laboratory “does”, and the method is updated every year with new values that define the results of susceptibility testing. YAWN!! It is one of those massive headaches laboratories have to undergo every year to make sure they adopt the new changes to the EUCAST method… it’s a bit of a chore really, lots of “subtle dullness” and paperwork etc.
However, something new and exciting is coming! Yes, these little things excite microbiologists… [Maybe “exciting” should also be a banned word along with interesting…] OK, OK, it is inappropriate to use exciting to describe changes to EUCAST reporting… but EUCAST are finally doing away with the intermediate susceptibility reporting… thank goodness!
You are still going to see susceptible and resistant, but the third type of report is going to be “susceptible at increased exposure”. Really!!! That’s not doing away with it, surely that’s just “tweaking” and semantics!!! Unfortunately, this doesn’t lend itself to an easy single letter for reporting, but locally we are going with S*, so that the isolate still looks susceptible.
Susceptible at increased exposure means that the bacterium is susceptible, but that an increased dose of antibiotic is needed; an increased dose can mean larger antibiotic doses and/or more frequent doses.
I do think this is better! No honest I do!!! It’s important to remember that nothing in medicine (and microbiology) is 100% accurate, and even though the laboratory might say a bacterium is susceptible the patient may not respond, and likewise the bacterium might be reported as resistant, but the patient gets better. This is because there are multiple factors in addition to laboratory testing that affect whether treatment is successful or not, including:
- Where is the infection? And does the antibiotic get into and have activity in the site of infection?
- The dose and frequency of the antibiotic
- The route of administration and whether the patient can absorb oral antibiotics
- The likelihood of the bacterium developing resistance during treatment
- Whether the dose of antibiotic is right for the patient’s body habitus (obesity is an increasingly common reason to fail therapy)
So, it’s important to interpret “susceptible at increased exposure” results as a guide to what antibiotics should treat a specific patient, rather than a guarantee that the treatment will work.
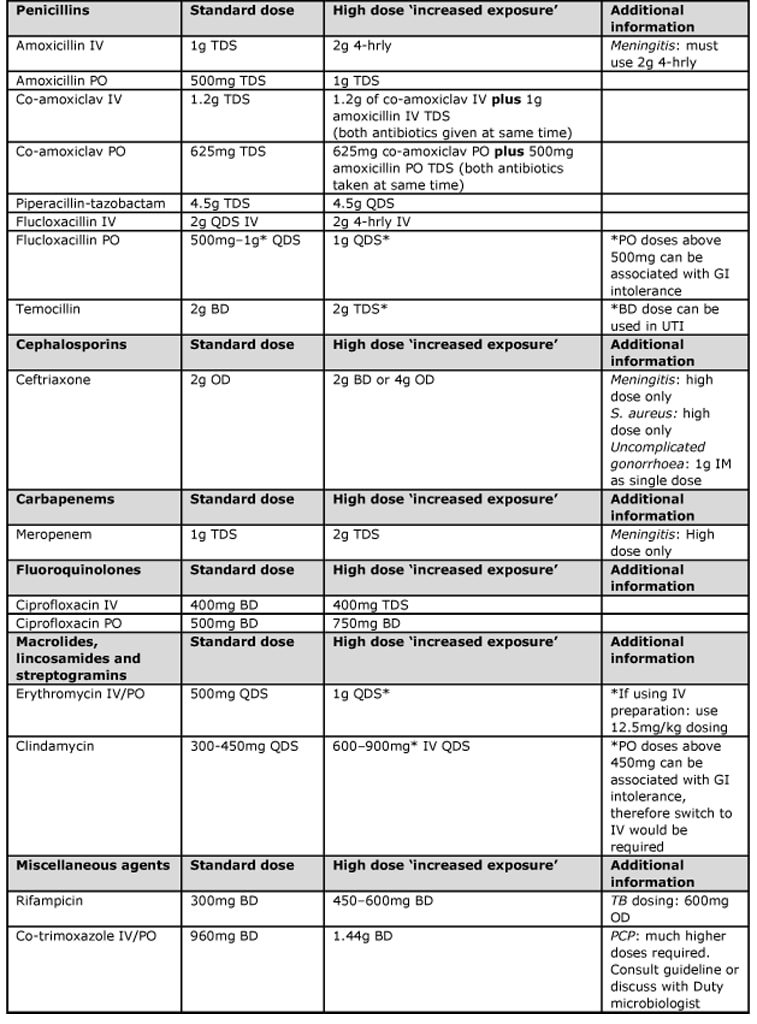
Different antibiotics have different ways of increasing the dose to correspond to an S* result. The table below shows the most important of these (assuming normal renal function, liver function and body mass index). For example, the normal dose of Amoxicillin is 1g TDS BUT the higher dose is 2g six times-a-day, for Temocillin the normal dose is 2g BD BUT the higher dose is 2g TDS, and for Ciprofloxacin the normal PO dose is 500mg BD BUT the higher dose is 750mg BD.
Click for larger image
I think this is a long-overdue change to the antimicrobial susceptibility reporting criteria. The combination of antimicrobial resistance and antimicrobial allergies can make it really difficult to treat some infections, and this change to proactively indicate higher dose treatment is very welcome.
This should give ward teams more options for the treatment of difficult infections, and after all none of us paid any attention to Intermediate results anyway! And maybe Microbiologists will be called on less to referee between people disagreeing about the meaning of intermediate results.
This should give ward teams more options for the treatment of difficult infections, and after all none of us paid any attention to Intermediate results anyway! And maybe Microbiologists will be called on less to referee between people disagreeing about the meaning of intermediate results.
 RSS Feed
RSS Feed
