It’s great how popular my blog about Poldark’s putrid throat has become, if you do a Google search for Poldark’s putrid throat it is the number 1 hit. Who says microbiology isn’t popular…? I have been asked by Jessica, who has read the Poldark blog, whether scarlet fever could have been the cause instead of diphtheria. So let’s consider this further, and explore the differential diagnosis of 18th Century Poldark’s putrid throat in more detail and why I came to the conclusion that it was diphtheria.
In order to do this I will first put Ross and Demelza Poldark’s daughter into a modern clinical scenario and then show how the historical perspective changes the possible diagnosis.
All we know at the beginning is that the child has a high fever, sore throat and is unwell. Very vague but it’s a start. What would be the very broad differential diagnosis for this child’s illness in today’s hospitals?
My method for producing a differential diagnosis is to use the following list in order, and then to fit a system-based approach afterwards:
Then the systems: respiratory, cardiovascular, neurological, genitourinary, gastrointestinal, skin, bone and joint can be considered under each heading.
The differential diagnosis of a high fever and sore throat in a young child being admitted today in a UK hospital might include:
All we know at the beginning is that the child has a high fever, sore throat and is unwell. Very vague but it’s a start. What would be the very broad differential diagnosis for this child’s illness in today’s hospitals?
My method for producing a differential diagnosis is to use the following list in order, and then to fit a system-based approach afterwards:
- Life-threatening conditions
- Common conditions
- Uncommon conditions
Then the systems: respiratory, cardiovascular, neurological, genitourinary, gastrointestinal, skin, bone and joint can be considered under each heading.
The differential diagnosis of a high fever and sore throat in a young child being admitted today in a UK hospital might include:
- Life-threatening conditions : epiglottitis, pertussis (whooping cough)
- Common: non-specific viral upper respiratory tract infection, croup, tonsillitis, scarlet fever
- Uncommon: diphtheria, Kawasaki’s disease, measles
This differential would be modified by taking a further history from the parents of the child, which includes taking an immunisation history. From our differential diagnosis the conditions which should be prevented by the primary course of childhood immunisations are: Haemophilus influenzae type b (abbreviated to Hib) epiglottitis, pertussis, diphtheria and measles. I have left epiglottitis and pertussis in the modern differential diagnosis because epiglottitis can be caused by bacteria other than Hib (e.g. Group A Beta-haemolytic streptococcus, Staphylococcus aureus) and pertussis immunity from vaccination weakens by school age and so it is still able to circulate in the community.
The immunisation history is important when putting the differential diagnosis of fever and sore throat into the historical context of Poldark’s 18th Century Cornwall. Not only were vaccines not available but the bacterial and viral causes of diseases had not even been discovered! So in this historical context our differential of a high fever and sore throat would include:
The same differential diagnosis would apply to countries with low vaccine availability or coverage. It is still important to remember this even in the UK as patients from Eastern Europe and the former Soviet States, who have not been vaccinated, may present to the NHS.
So let’s now look at the 18th Century child’s symptoms in more detail. Not only does she have the fever and sore throat but she is also having difficulty breathing. The problem seems to be the actual movement of air in and out which implies a narrowing of the pharynx, epiglottis or trachea. The airway narrowing allows us to exclude pertussis, measles, non-specific viral URTI, scarlet fever and Kawasaki’s disease, as none of these present with airway narrowing. Added to this there is no spasmodic cough so pertussis is even more unlikely and the absence of a rash makes scarlet fever and measles very unlikely indeed (in scarlet fever the rash is typically a diffuse “sunburn style” rash see the blog on scarlet fever).
So our historical differential diagnosis might now look something like:
Croup can be excluded by careful attention to the child’s breathing pattern; croup causes a barking cough, sounding much like a seal, and the child is not usually that unwell even if they sound dreadful! This leaves us with 3 possible diagnoses which can be differentiated by a careful and I really mean careful examination of the child. If the child is very unwell and really struggling to breath then any examination should only be done with the ability to perform an emergency tracheostomy just in case the swollen airway shuts off completely. If in doubt get help before examining the child’s throat!
The immunisation history is important when putting the differential diagnosis of fever and sore throat into the historical context of Poldark’s 18th Century Cornwall. Not only were vaccines not available but the bacterial and viral causes of diseases had not even been discovered! So in this historical context our differential of a high fever and sore throat would include:
- Life-threatening conditions: diphtheria, epiglottitis, pertussis (whooping cough), measles
- Common: non-specific viral upper respiratory tract infection (URTI), croup, tonsillitis, scarlet fever
- Uncommon: Kawasaki’s disease
The same differential diagnosis would apply to countries with low vaccine availability or coverage. It is still important to remember this even in the UK as patients from Eastern Europe and the former Soviet States, who have not been vaccinated, may present to the NHS.
So let’s now look at the 18th Century child’s symptoms in more detail. Not only does she have the fever and sore throat but she is also having difficulty breathing. The problem seems to be the actual movement of air in and out which implies a narrowing of the pharynx, epiglottis or trachea. The airway narrowing allows us to exclude pertussis, measles, non-specific viral URTI, scarlet fever and Kawasaki’s disease, as none of these present with airway narrowing. Added to this there is no spasmodic cough so pertussis is even more unlikely and the absence of a rash makes scarlet fever and measles very unlikely indeed (in scarlet fever the rash is typically a diffuse “sunburn style” rash see the blog on scarlet fever).
So our historical differential diagnosis might now look something like:
- Life-threatening conditions: diphtheria, epiglottitis
- Common: croup, tonsillitis
Croup can be excluded by careful attention to the child’s breathing pattern; croup causes a barking cough, sounding much like a seal, and the child is not usually that unwell even if they sound dreadful! This leaves us with 3 possible diagnoses which can be differentiated by a careful and I really mean careful examination of the child. If the child is very unwell and really struggling to breath then any examination should only be done with the ability to perform an emergency tracheostomy just in case the swollen airway shuts off completely. If in doubt get help before examining the child’s throat!

Click for larger image
Examine children carefully!
Examine children carefully!
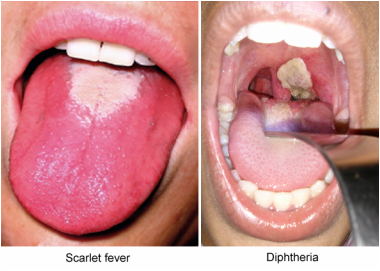
In epiglottitis the pharynx looks normal or a little red (but no putrid throat) instead the epiglottis looks cherry red, swollen and may obstruct the opening of the trachea. In tonsillitis the tonsils are red and swollen and possibly covered in pus but they rarely swell enough to occlude the pharynx. In diphtheria there is usually a grey “Clingfilm” membrane adherent to the pharynx, the cervical lymph nodes are very enlarged leading to a “bull neck” appearance and there are often other acute symptoms related to the systemic absorption of toxin from the bacterium e.g. myocarditis. Whilst myocarditis can occur in Group A Beta-haemolytic streptococcal tonsillitis it is usually a later finding and associated with the development of rheumatic heart disease whereas in diphtheria it is acute. Patients with diphtheria are usually much more unwell and death can occur very quickly.
So for Poldark we really have a choice between diphtheria and severe tonsillitis and given the symptoms of "putrid throat", severe life-threatening disease, contagiousness and cardiac symptoms, we can narrow our differential down to a definitive diagnosis… diphtheria. If you want to know more about diphtheria see the original blog on Poldark’s Putrid Throat. If you search hard enough on the internet too you’ll find an interview with a BBC producer who says they based the story on diphtheria! Being able to differentiate the diagnosis yourself though is surely more satisfying. :-)
So that’s the process of exploring a differential diagnosis and how I came to the conclusion that Poldark’s Putrid Throat was diphtheria. Jessica was right, scarlet fever was considered as part of the differential, but on balance I believe that diphtheria was the culprit.
The art of developing a differential diagnosis appears to have gone out of day-to-day medicine and I think we should try and bring it back. Most of the time I see doctors trying to pinpoint a single diagnosis at the point the patient is admitted without waiting for further information from the history, examination and investigations. I think this is a mistake and possibly wrong, it takes away our diagnostic skills. As a result no one questions whether the initial diagnosis is right or wrong and therefore a patient can end up being treated for one infection when they actually have another. Keep an open mind; it is good practice and ultimately it makes for safer medicine and it’s certainly more fulfilling.
So for Poldark we really have a choice between diphtheria and severe tonsillitis and given the symptoms of "putrid throat", severe life-threatening disease, contagiousness and cardiac symptoms, we can narrow our differential down to a definitive diagnosis… diphtheria. If you want to know more about diphtheria see the original blog on Poldark’s Putrid Throat. If you search hard enough on the internet too you’ll find an interview with a BBC producer who says they based the story on diphtheria! Being able to differentiate the diagnosis yourself though is surely more satisfying. :-)
So that’s the process of exploring a differential diagnosis and how I came to the conclusion that Poldark’s Putrid Throat was diphtheria. Jessica was right, scarlet fever was considered as part of the differential, but on balance I believe that diphtheria was the culprit.
The art of developing a differential diagnosis appears to have gone out of day-to-day medicine and I think we should try and bring it back. Most of the time I see doctors trying to pinpoint a single diagnosis at the point the patient is admitted without waiting for further information from the history, examination and investigations. I think this is a mistake and possibly wrong, it takes away our diagnostic skills. As a result no one questions whether the initial diagnosis is right or wrong and therefore a patient can end up being treated for one infection when they actually have another. Keep an open mind; it is good practice and ultimately it makes for safer medicine and it’s certainly more fulfilling.
 RSS Feed
RSS Feed
