It’s that time of year again, in UK hospitals healthcare staff are walking the wards with a slightly sore left arm sucking on a boiled sweet lollipop… yep, it’s flu vaccine season!
Every year the NHS tries to vaccinate as many of the frontline healthcare staff as possible in order to prevent outbreaks of influenza in our hospitals. In addition GPs are busy coaxing as many of the over 65 year olds as possible to get vaccinated before “flu season” starts. This is in addition to the routine flu vaccination of 2-3 year old children in reception classes and Years 1-4 at school (age 4-8 years).
Every year the NHS tries to vaccinate as many of the frontline healthcare staff as possible in order to prevent outbreaks of influenza in our hospitals. In addition GPs are busy coaxing as many of the over 65 year olds as possible to get vaccinated before “flu season” starts. This is in addition to the routine flu vaccination of 2-3 year old children in reception classes and Years 1-4 at school (age 4-8 years).

Why do we do this?
Worldwide there are about a billion cases of influenza every year, with up to 500,000 deaths. In the UK there are over a million cases of influenza in a normal influenza season. It is suggested by the Department of Health and Public Health England that there are approximately 12,000 excess deaths in the UK per year from influenza but this figure is a bit controversial. The figure is based on looking at how many extra people per year die over the winter period, then estimating how many of these were “related to influenza”, either directly from influenza itself (probably only about 30-40 cases) or indirectly due to other diseases made worse by influenza e.g. ischaemic heart disease, chronic obstructive pulmonary disease, etc. Many Virologists and Epidemiologists think the influenza related death figure is actually far lower than 12,000, more realistically around 2,000-2,500, but these are all potentially vaccine preventable deaths.
Last year about 63% of healthcare staff in the NHS were vaccinated against influenza which was up from 51% the year before, but it’s still not that great a result. I find it a bit odd that healthcare staff don’t get vaccinated as there are some major benefits to being vaccinated:
To me it’s a bit of a “no-brainer”, all healthcare staff should be vaccinated unless they have a medical reason why not.
Worldwide there are about a billion cases of influenza every year, with up to 500,000 deaths. In the UK there are over a million cases of influenza in a normal influenza season. It is suggested by the Department of Health and Public Health England that there are approximately 12,000 excess deaths in the UK per year from influenza but this figure is a bit controversial. The figure is based on looking at how many extra people per year die over the winter period, then estimating how many of these were “related to influenza”, either directly from influenza itself (probably only about 30-40 cases) or indirectly due to other diseases made worse by influenza e.g. ischaemic heart disease, chronic obstructive pulmonary disease, etc. Many Virologists and Epidemiologists think the influenza related death figure is actually far lower than 12,000, more realistically around 2,000-2,500, but these are all potentially vaccine preventable deaths.
Last year about 63% of healthcare staff in the NHS were vaccinated against influenza which was up from 51% the year before, but it’s still not that great a result. I find it a bit odd that healthcare staff don’t get vaccinated as there are some major benefits to being vaccinated:
- You are less likely to develop influenza and become ill
- You are less likely to take influenza home and infect you family including elderly relatives who are more at risk of severe disease
- You are less likely to transmit influenza to uninfected vulnerable patients such as the elderly and immunosuppressed who might die from infection (1 in 3 people will not show any symptoms, but are infectious to others)
- You get a free lollipop!
To me it’s a bit of a “no-brainer”, all healthcare staff should be vaccinated unless they have a medical reason why not.
What’s in the vaccine?
The vaccine is made up of two types of inactivated Influenza A Virus and one type of Influenza B Virus; it is known as a trivalent vaccine as it has three components.
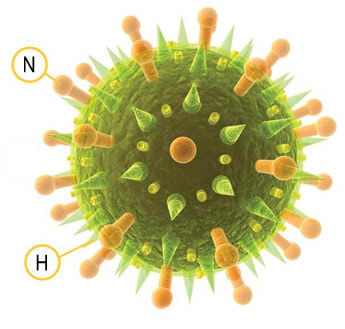
Each of the Influenza A Viruses have specific capsular proteins called haemagglutinin (H) and neuraminidase (N) and each of these H and Ns has a number which subdivides them further into type e.g. Influenza A Virus is a catch-all term for lots and lots of Influenza A Viruses including Influenza A Virus H1N1 or Influenza A Virus H3N2 or Influenza A Virus H7N2 for example, but they are still all Influenza A Virus.
To make things even more complicated there are many different versions of H1N1 (e.g. A/Michigan/45/2015pdm09–like virus) or H3N2 (A/Hong Kong/4801/2014-like virus)… OMG… you get the picture, there are lots of different influenza viruses out there! The vaccine is usually made up of an H1N1 and an H2N3 Influenza A Virus. Influenza B Virus does not have this designation into H and N types.
The vaccine is made up of two types of inactivated Influenza A Virus and one type of Influenza B Virus; it is known as a trivalent vaccine as it has three components.
Each of the Influenza A Viruses have specific capsular proteins called haemagglutinin (H) and neuraminidase (N) and each of these H and Ns has a number which subdivides them further into type e.g. Influenza A Virus is a catch-all term for lots and lots of Influenza A Viruses including Influenza A Virus H1N1 or Influenza A Virus H3N2 or Influenza A Virus H7N2 for example, but they are still all Influenza A Virus.
To make things even more complicated there are many different versions of H1N1 (e.g. A/Michigan/45/2015pdm09–like virus) or H3N2 (A/Hong Kong/4801/2014-like virus)… OMG… you get the picture, there are lots of different influenza viruses out there! The vaccine is usually made up of an H1N1 and an H2N3 Influenza A Virus. Influenza B Virus does not have this designation into H and N types.
What types of vaccine are available in the UK?
In the UK we currently have 2 types of vaccine, injectable and nasal spray:
How do vaccine companies choose what type of H and N to use?
The reason why having influenza does not protect you from getting influenza again and why there is a need for yearly vaccination is that the influenza viruses are very good at changing their genetic makeup. There are two types of genetic change; antigenic drift and antigenic shift.
As a result of drift and shift, vaccine companies have to try and guess which type of virus might cause the next seasonal influenza or even pandemic. It takes about six months to manufacture flu vaccine and so the guessing has to begin a long time in advance of actually knowing what strains of virus will be around and so sometimes the guesses are not as accurate as one might hope.
I call it guessing but that’s not really fair. The choice of vaccine strains is based on extensive study by the World Health Organization (WHO) of what strains are circulating in the populations of the alternative global hemispheres, so our vaccine in the Northern hemisphere is based on what is going on 6-12 months earlier in the Southern hemisphere, and vice versa. Sometimes the vaccine is well matched and we see much less influenza that year, sometimes it is not so well matched and we get a lot of influenza. In some years there is complete antigenic shift and we get a pandemic… this is what happened in 2009 with so called “Swine Flu”.
Last year the vaccine in the UK was not that well matched to the circulating strains. This is because the seasonal influenza strain last year was caused by a virus which only partly matched the vaccine components. Both the infection strains and the vaccine strains were both H1N1 and H2N3 but they didn’t match well enough for the vaccine to be effective.
Last year’s vaccine only prevented about 40% of influenza in those who were vaccinated. Not only this but this was also only in people under 65 years old; it was of no benefit in the over 65 year olds. Worryingly the high risk over 65 year olds got no benefit from their vaccine, probably because the poorly matched vaccine related antibody in these elderly patients did not react at all to the circulating strains of influenza virus.
So this raises the question of why has no one developed an influenza vaccine against all influenza viruses? Well they just have…!
INVICTUS
The new vaccine has been developed by Vaccitech, a spin-out company from the University of Oxford’s Jenner Institute. A clinical study is under way to investigate the effectiveness of a new type of influenza vaccine. The study is called INVICTUS (Improved Novel VaccIne CombinaTion InflUenza Study… invictus may mean “unconquered” in Latin but I think this is stretching an acronym to its limit!).
The new vaccine doesn’t use the old fashioned H and N proteins to trigger the immune response; instead it uses the core proteins of the virus which actually don’t change much between different types of Influenza A Virus. The new vaccine stimulates a T cell response rather than the normal B cell antibody response of the current vaccines. This is important because the B cell antibody response is targeted at virally infected cells whereas the T cell response should also target free virus outside of the cells even in the absence of antibodies i.e. against a strain of virus the immune system has never seen before. If this really works then this vaccine should be very effective at reducing influenza every year, irrespective of the type of circulating virus.
So what are the drawbacks?
Well as this vaccine is only just going in to a phase 2 randomized and blinded study, these are not yet documented so we’ll need to wait until this study is published. However the main drawback I can foresee is that nowhere in the pre-study literature does it suggest that the vaccine protects against Influenza B Virus. This is disappointing as people will still be able to catch “Flu” from Influenza B Virus even if they have had their Flu jab; this may cause a marketing issue as the general public won’t necessarily understand why their “one-off” flu jab is not protecting them! However, if the vaccine works as the manufacturers hope and rids the population of Influenza A Virus (which normally causes most of the illness and death each year) this slight omission may not be such a severe drawback that it will stop the vaccine being used by governments.
So the INVICTUS trial has been launched and active recruitment of about 2000 volunteers over the age of 65 years has begun. Volunteers will receive either the current injectable vaccine PLUS the INVICTUS vaccine or the current injectable vaccine PLUS a placebo. The trial is taking place in Oxfordshire and Berkshire in the UK and I’m looking forward to seeing how it gets on.
So have you had you flu vaccine yet? No! Why not? Go on treat yourself to a lollipop and get a free vaccine at the same time. This is your yearly NHS treat…but be warned, with INVICTUS on the cards even a yearly lollipop looks likely to be taken away from us!
In the UK we currently have 2 types of vaccine, injectable and nasal spray:
- The injectable form is usually given into the deltoid muscle of the left arm (hence the slightly sore arm). This vaccine is not a live vaccine so you cannot catch flu from it, although you often hear patients telling stories of how their vaccine “gave them Flu”. It works by stimulating the immune system to produce antibodies against the H and N proteins.
- The nasal spray vaccine contains live attenuated virus; H1N1, H3N2 as well as two Influenza B Viruses. The nasal spray is squirted once up each nostril and is very well tolerated by children. As a live virus the nasal spray vaccine works by causing a mild localised influenza infection in the nose which then triggers the immune system to produce antibodies against the four different viruses. It should not be given to people with immune deficiencies as they could possibly develop full blown infection even from the weakened vaccine virus.
How do vaccine companies choose what type of H and N to use?
The reason why having influenza does not protect you from getting influenza again and why there is a need for yearly vaccination is that the influenza viruses are very good at changing their genetic makeup. There are two types of genetic change; antigenic drift and antigenic shift.
- Drift is due to small changes in the genetics of the virus, meaning people become infected but as they have experienced a similar virus their bodies can recognise a large element of the new virus. Relatively few people are infected and they have milder symptoms. This is seasonal flu, which genetically changes slightly but continuously
- Shift occurs when the virus acquires new genes from a different Influenza Virus. This creates a new virus people have not been exposed to yet, capable of causing a pandemic. Pandemic “Swine Flu” and “Bird Flu” are examples of antigenic shift in an animal, e.g. the pig had both human and avian flu and genes swapped between them to create a new Influenza Virus. These pandemic viruses tend to become the “next” seasonal virus after the population has been exposed
As a result of drift and shift, vaccine companies have to try and guess which type of virus might cause the next seasonal influenza or even pandemic. It takes about six months to manufacture flu vaccine and so the guessing has to begin a long time in advance of actually knowing what strains of virus will be around and so sometimes the guesses are not as accurate as one might hope.
I call it guessing but that’s not really fair. The choice of vaccine strains is based on extensive study by the World Health Organization (WHO) of what strains are circulating in the populations of the alternative global hemispheres, so our vaccine in the Northern hemisphere is based on what is going on 6-12 months earlier in the Southern hemisphere, and vice versa. Sometimes the vaccine is well matched and we see much less influenza that year, sometimes it is not so well matched and we get a lot of influenza. In some years there is complete antigenic shift and we get a pandemic… this is what happened in 2009 with so called “Swine Flu”.
Last year the vaccine in the UK was not that well matched to the circulating strains. This is because the seasonal influenza strain last year was caused by a virus which only partly matched the vaccine components. Both the infection strains and the vaccine strains were both H1N1 and H2N3 but they didn’t match well enough for the vaccine to be effective.
Last year’s vaccine only prevented about 40% of influenza in those who were vaccinated. Not only this but this was also only in people under 65 years old; it was of no benefit in the over 65 year olds. Worryingly the high risk over 65 year olds got no benefit from their vaccine, probably because the poorly matched vaccine related antibody in these elderly patients did not react at all to the circulating strains of influenza virus.
So this raises the question of why has no one developed an influenza vaccine against all influenza viruses? Well they just have…!
INVICTUS
The new vaccine has been developed by Vaccitech, a spin-out company from the University of Oxford’s Jenner Institute. A clinical study is under way to investigate the effectiveness of a new type of influenza vaccine. The study is called INVICTUS (Improved Novel VaccIne CombinaTion InflUenza Study… invictus may mean “unconquered” in Latin but I think this is stretching an acronym to its limit!).
The new vaccine doesn’t use the old fashioned H and N proteins to trigger the immune response; instead it uses the core proteins of the virus which actually don’t change much between different types of Influenza A Virus. The new vaccine stimulates a T cell response rather than the normal B cell antibody response of the current vaccines. This is important because the B cell antibody response is targeted at virally infected cells whereas the T cell response should also target free virus outside of the cells even in the absence of antibodies i.e. against a strain of virus the immune system has never seen before. If this really works then this vaccine should be very effective at reducing influenza every year, irrespective of the type of circulating virus.
So what are the drawbacks?
Well as this vaccine is only just going in to a phase 2 randomized and blinded study, these are not yet documented so we’ll need to wait until this study is published. However the main drawback I can foresee is that nowhere in the pre-study literature does it suggest that the vaccine protects against Influenza B Virus. This is disappointing as people will still be able to catch “Flu” from Influenza B Virus even if they have had their Flu jab; this may cause a marketing issue as the general public won’t necessarily understand why their “one-off” flu jab is not protecting them! However, if the vaccine works as the manufacturers hope and rids the population of Influenza A Virus (which normally causes most of the illness and death each year) this slight omission may not be such a severe drawback that it will stop the vaccine being used by governments.
So the INVICTUS trial has been launched and active recruitment of about 2000 volunteers over the age of 65 years has begun. Volunteers will receive either the current injectable vaccine PLUS the INVICTUS vaccine or the current injectable vaccine PLUS a placebo. The trial is taking place in Oxfordshire and Berkshire in the UK and I’m looking forward to seeing how it gets on.
So have you had you flu vaccine yet? No! Why not? Go on treat yourself to a lollipop and get a free vaccine at the same time. This is your yearly NHS treat…but be warned, with INVICTUS on the cards even a yearly lollipop looks likely to be taken away from us!
 RSS Feed
RSS Feed
