The Microbiologist sighed; yet another telephone call about poo. Didn’t they know it was nearly lunch time? This time the patient was a 4 year old who had had diarrhoea associated with cramping abdominal pain for a week. A stool sample had been sent to the laboratory and a result was available… the GP wanted to know what antibiotic to start as the child was having a birthday party next week and the parents wanted to take him and his friends to the local water park. The Microbiologist quickly turned into the “fun police” and strongly advised against both antibiotics and swimming! "Oh they will be disappointed!" said the GP.

Enjoy Half-term!
In the UK, when you walk into a water park (full of slides, whirlpools and jets of warm water) you can’t help but notice the signs everywhere telling you that if either you or your children have had diarrhoea then don’t go in the water. The reason is obvious; “if you have infectious diarrhoea nobody wants you to share it with anyone else”. But which microorganism is the main cause for concern, how long are you infectious for and how do you know if you have it?
In the case of water parks and swimming pools, the microorganism which causes most concern is Cryptosporium spp.; it is commonly known as “Craptosporidium” by Microbiologists because of the large outbreaks of diarrhoea it can cause.
What is Cryptosporium spp.?
There are over 20 different species of Cryptosporidium but the two types responsible for causing infections in humans are C. parvum and C. hominis. The other species are specific to certain animals e.g. C. felis in cats, C. muris in mice, C. canis in dogs… you get the idea…
Cryptosporidium spp. are found all over the world, in both developing and developed countries. Spread is via the faecal-oral route and therefore poor sanitation is a major risk factor for infection. It is estimated that the infectious dose of Cryptosporium spp. is only 10-50 oocysts (eggs) and that an infected person can excrete billions of oocysts whilst infected; so it is very easily spread to other people. Infection is most common in children where it causes about 3% of all diarrhoea in developed countries and 10% in developing countries.
In the case of water parks and swimming pools, the microorganism which causes most concern is Cryptosporium spp.; it is commonly known as “Craptosporidium” by Microbiologists because of the large outbreaks of diarrhoea it can cause.
What is Cryptosporium spp.?
There are over 20 different species of Cryptosporidium but the two types responsible for causing infections in humans are C. parvum and C. hominis. The other species are specific to certain animals e.g. C. felis in cats, C. muris in mice, C. canis in dogs… you get the idea…
Cryptosporidium spp. are found all over the world, in both developing and developed countries. Spread is via the faecal-oral route and therefore poor sanitation is a major risk factor for infection. It is estimated that the infectious dose of Cryptosporium spp. is only 10-50 oocysts (eggs) and that an infected person can excrete billions of oocysts whilst infected; so it is very easily spread to other people. Infection is most common in children where it causes about 3% of all diarrhoea in developed countries and 10% in developing countries.

How does cryptosporidiosis present?
Whilst C. parvum and C. hominis tend to cause a gastrointestinal illness with diarrhoea and abdominal pain associated with a mild fever, up to 30% of patients are asymptomatic! Meaning they might be swimming unaware of the dangers they pose.
The incubation period is normally between 7-10 days. Symptoms usually resolve within 2 weeks although oocysts can be excreted in stool for weeks to months. Hence the cancellation of the swim party!
Severe infection with significant fluid loss and dehydration can occur, especially in immunosuppressed patients including: Human Immunodeficiency Virus (HIV), transplant recipients, hypogammaglobulinaemia and immunosuppressing drugs such as cancer chemotherapy.
So why the fun police’s attack on swimming pools?!? (Meanies!!)
Most cases of cryptosporidiosis are associated with contaminated water. Cryptosporidium spp. can be found in 65-95% of environmental surface water and these parasites can survive there for months. Once they get in to a water source they are very difficult to kill, as they are inherently resistant to many disinfectants and are not always removed by filters. Cases either occur from contaminated drinking water (don’t ignore those “boil your water” notices from the water company!) or in the UK more commonly… swimming pools.
In the UK there have been a number of swimming pool related outbreaks with 18 significant outbreaks reported between 1989 and 1999. I particularly remember the 54 cases thought to be related to the Temple Cowley swimming pool in Oxford… maybe it sticks in my mind as my wife used to use the gym and pool facilities at the time!
The most infamous outbreak of drinking water related cryptosporidiosis happened in Milwaukee in the USA in 1993 when about 403,000 people were infected via the city water supply which was contaminated with C. parvum. It is thought that this figure may actually be an underestimate as this is only about 25% of the population of Milwaukee in 1993 and there have been some studies that showed that antibody evidence of exposure during this time may have been as high as 80-85% of the population, whoops that’s a lot of people!
How is cryptosporidiosis diagnosed?
Cryptosporidium spp. cannot be grown in the laboratory. The most common method for detection in the UK is microscopy with PCR starting to become more widely available.
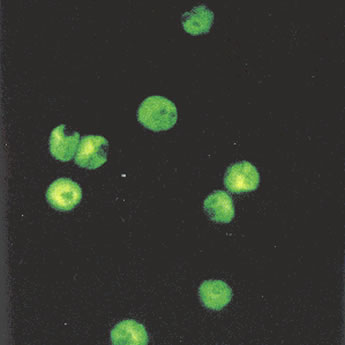
Most laboratories in the UK will routinely and literally “look” for Cryptosporidium spp. in stool samples from patients with diarrhoea in the community. If your laboratory does not then you will need to give good clinical information on the request form, e.g. prolonged diarrhoea or suspect water-borne infection, and specifically ask for a test for ova, cysts and parasites (OCP). The microscopy method used to look for Cryptosporidium spp. is a modified acid fast stain, a bit like the stain used to look for Mycobacterium spp., with auramine stains and UV light being commonly used to make seeing the parasites easier.
Whilst C. parvum and C. hominis tend to cause a gastrointestinal illness with diarrhoea and abdominal pain associated with a mild fever, up to 30% of patients are asymptomatic! Meaning they might be swimming unaware of the dangers they pose.
The incubation period is normally between 7-10 days. Symptoms usually resolve within 2 weeks although oocysts can be excreted in stool for weeks to months. Hence the cancellation of the swim party!
Severe infection with significant fluid loss and dehydration can occur, especially in immunosuppressed patients including: Human Immunodeficiency Virus (HIV), transplant recipients, hypogammaglobulinaemia and immunosuppressing drugs such as cancer chemotherapy.
So why the fun police’s attack on swimming pools?!? (Meanies!!)
Most cases of cryptosporidiosis are associated with contaminated water. Cryptosporidium spp. can be found in 65-95% of environmental surface water and these parasites can survive there for months. Once they get in to a water source they are very difficult to kill, as they are inherently resistant to many disinfectants and are not always removed by filters. Cases either occur from contaminated drinking water (don’t ignore those “boil your water” notices from the water company!) or in the UK more commonly… swimming pools.
In the UK there have been a number of swimming pool related outbreaks with 18 significant outbreaks reported between 1989 and 1999. I particularly remember the 54 cases thought to be related to the Temple Cowley swimming pool in Oxford… maybe it sticks in my mind as my wife used to use the gym and pool facilities at the time!
The most infamous outbreak of drinking water related cryptosporidiosis happened in Milwaukee in the USA in 1993 when about 403,000 people were infected via the city water supply which was contaminated with C. parvum. It is thought that this figure may actually be an underestimate as this is only about 25% of the population of Milwaukee in 1993 and there have been some studies that showed that antibody evidence of exposure during this time may have been as high as 80-85% of the population, whoops that’s a lot of people!
How is cryptosporidiosis diagnosed?
Cryptosporidium spp. cannot be grown in the laboratory. The most common method for detection in the UK is microscopy with PCR starting to become more widely available.
Most laboratories in the UK will routinely and literally “look” for Cryptosporidium spp. in stool samples from patients with diarrhoea in the community. If your laboratory does not then you will need to give good clinical information on the request form, e.g. prolonged diarrhoea or suspect water-borne infection, and specifically ask for a test for ova, cysts and parasites (OCP). The microscopy method used to look for Cryptosporidium spp. is a modified acid fast stain, a bit like the stain used to look for Mycobacterium spp., with auramine stains and UV light being commonly used to make seeing the parasites easier.
PCR is more sensitive than microscopy for diagnosing cryptosporidiosis but it is not yet universally available in the UK due to cost. PCR has the added advantage of being able to differentiate different species as well as genetically compare isolates in the outbreak setting.
In the UK it is really important that all positive samples are sent to the Enteric Reference Laboratory for Public Health England (PHE) as well as being notified to the PHE. This is because of the potential for large water-borne outbreaks (just think of how many kids are in a swimming pool at half-term!) and therefore there is a significant risk to public health if outbreaks are not spotted and dealt with early.
How is cryptosporidiosis treated?
Infections in patients with normal immune systems are self-limiting and specific treatment is not indicated although it can take weeks for the symptoms to settle. The immune system is better at removing Cryptosporium spp. than antibiotic treatments. However, antibiotics are advised in immunosuppressed patients with chronic or severe infection (Nitazoxanide 500mg BD for at least 2 weeks) as well as supportive care with fluid rehydration. Chronic severe infection in these patient groups is potentially life-threatening due to fluid and electrolyte imbalances and nutritional failure. Nitazoxanide on its own is often not that effective and it is important to try and reverse the immunosuppression as well e.g. with antiretrovirals in HIV infection.
How can cryptosporidiosis be prevented?
The most important factor in preventing cryptosporidiosis is to stop people who may be infectious from swimming in pools and thereby spreading the infection. This means advising members of the public that if they have diarrhoea or have had diarrhoea within the preceding 2 weeks they should not swim in swimming pools.
Those responsible for ensuring the hygiene of swimming pools should also have a filtration system in place that is effective at removing cryptosporium oocysts from contaminated water. Chlorination alone is not enough as the oocysts are resistant to the normal levels of chlorine used in pools.
Water sources used for drinking water should be protected from contamination with oocysts, water companies must ensure that sewerage cannot contaminate drinking water supplies and that water for drinking has been filtered before consumption. During outbreaks the public are advised to boil or filter their water (absolute retention rating of 5 microns or less) as these are effective methods for killing or removing the oocysts.
So the GP was strongly advised to inform the parents that the child could not go swimming and should be reassured that their child’s symptoms would eventually settle without antibiotics. Whilst authorising results later that day the Microbiologist kept a close eye out for more cases of cryptosporidium from the same area but none were apparent and so the Microbiologist was also reassured that there was no obvious outbreak going on at the moment. The sample was sent to the Enteric Reference Laboratory for PHE and the result was notified to the PHE by both the laboratory and GP, as both have a legal responsibility to do so.
In the UK it is really important that all positive samples are sent to the Enteric Reference Laboratory for Public Health England (PHE) as well as being notified to the PHE. This is because of the potential for large water-borne outbreaks (just think of how many kids are in a swimming pool at half-term!) and therefore there is a significant risk to public health if outbreaks are not spotted and dealt with early.
How is cryptosporidiosis treated?
Infections in patients with normal immune systems are self-limiting and specific treatment is not indicated although it can take weeks for the symptoms to settle. The immune system is better at removing Cryptosporium spp. than antibiotic treatments. However, antibiotics are advised in immunosuppressed patients with chronic or severe infection (Nitazoxanide 500mg BD for at least 2 weeks) as well as supportive care with fluid rehydration. Chronic severe infection in these patient groups is potentially life-threatening due to fluid and electrolyte imbalances and nutritional failure. Nitazoxanide on its own is often not that effective and it is important to try and reverse the immunosuppression as well e.g. with antiretrovirals in HIV infection.
How can cryptosporidiosis be prevented?
The most important factor in preventing cryptosporidiosis is to stop people who may be infectious from swimming in pools and thereby spreading the infection. This means advising members of the public that if they have diarrhoea or have had diarrhoea within the preceding 2 weeks they should not swim in swimming pools.
Those responsible for ensuring the hygiene of swimming pools should also have a filtration system in place that is effective at removing cryptosporium oocysts from contaminated water. Chlorination alone is not enough as the oocysts are resistant to the normal levels of chlorine used in pools.
Water sources used for drinking water should be protected from contamination with oocysts, water companies must ensure that sewerage cannot contaminate drinking water supplies and that water for drinking has been filtered before consumption. During outbreaks the public are advised to boil or filter their water (absolute retention rating of 5 microns or less) as these are effective methods for killing or removing the oocysts.
So the GP was strongly advised to inform the parents that the child could not go swimming and should be reassured that their child’s symptoms would eventually settle without antibiotics. Whilst authorising results later that day the Microbiologist kept a close eye out for more cases of cryptosporidium from the same area but none were apparent and so the Microbiologist was also reassured that there was no obvious outbreak going on at the moment. The sample was sent to the Enteric Reference Laboratory for PHE and the result was notified to the PHE by both the laboratory and GP, as both have a legal responsibility to do so.
 RSS Feed
RSS Feed
