
I was recently asked for advice about a patient who had severe community acquired pneumonia (CAP), the team looking after him were concerned as despite 5 days of IV Teicoplanin and Levofloxacin (he had a history of severe penicillin allergy) his blood inflammatory markers had not started to come down. Strange, I thought as this is normally a good combination for CAP.
The team was asked to check that the diagnosis was correct. There was no new infection, which might be causing a problem and a review of his old chest x-ray confirmed pneumonia. They had followed the hospital antibiotic guidelines so knew the choice of antibiotic was correct and the antibiotics had definitely been given and at appropriate doses. They were understandably at a loss as to what might be going on, so I wandered up to the ward.
I retook the history of presenting complaint and did not elicit any other potential complications but my examination of the patient’s chest suggested the presence of fluid in the chest (decreased expansion, absent breath sounds, dullness to percussion). This raised the possibility of an empyema which would be consistent with CAP not responding to the current antibiotics.
Why was “correct” treatment failing?
1. Most antibiotics do not get into the pleural space in high concentrations
2. The acidic nature of empyema pus further degrades the antibiotic making it less effective
3. The pus itself may contain an organism, which does not respond to the current combination of antibiotics
The team were advised to drain the pleural fluid and send the pus to the lab. A CT scan, confirmed an empyema, and thick pus was drained by the radiologist. No organisms were seen on microscopy of the pus sample however the patient was changed to a combination of antibiotics with better penetration into the pleural space, IV Teicoplanin and Clindamycin. The essential component was the drainage of the empyema which unless done will prevent the antibiotics from working properly.
Why both antibiotics?
Clindamycin is good at getting into the pleural space and covers anaerobes. However the Gram-positive activity of Clindamycin is unreliable therefore Teicoplanin is added.
By the following day the patient was feeling much better due to the 1 litre of pus that was no longer in his chest. The culture result, of the pus sample, grew a bacteria called Fusobacterium necrophorum, which in Latin means “spindly bacterium of death”. What a great name!
Fusobacterium sp. are Gram-negative anaerobic bacteria usually found as part of the upper gastrointestinal and respiratory tract. They are an unusual cause of CAP but do occasionally occur, usually in middle-aged men with a history of recent high alcohol intake (presumably this means they aspirate some of their upper gastrointestinal tract bacteria because the overuse of alcohol prevents them from protecting their airway). The condition is known as
Necrobacillosis and presents as a particularly severe form of pneumonia requiring long courses of antibiotics such as Penicillin, Metronidazole or Clindamycin.
I retook the history of presenting complaint and did not elicit any other potential complications but my examination of the patient’s chest suggested the presence of fluid in the chest (decreased expansion, absent breath sounds, dullness to percussion). This raised the possibility of an empyema which would be consistent with CAP not responding to the current antibiotics.
Why was “correct” treatment failing?
1. Most antibiotics do not get into the pleural space in high concentrations
2. The acidic nature of empyema pus further degrades the antibiotic making it less effective
3. The pus itself may contain an organism, which does not respond to the current combination of antibiotics
The team were advised to drain the pleural fluid and send the pus to the lab. A CT scan, confirmed an empyema, and thick pus was drained by the radiologist. No organisms were seen on microscopy of the pus sample however the patient was changed to a combination of antibiotics with better penetration into the pleural space, IV Teicoplanin and Clindamycin. The essential component was the drainage of the empyema which unless done will prevent the antibiotics from working properly.
Why both antibiotics?
Clindamycin is good at getting into the pleural space and covers anaerobes. However the Gram-positive activity of Clindamycin is unreliable therefore Teicoplanin is added.
By the following day the patient was feeling much better due to the 1 litre of pus that was no longer in his chest. The culture result, of the pus sample, grew a bacteria called Fusobacterium necrophorum, which in Latin means “spindly bacterium of death”. What a great name!
Fusobacterium sp. are Gram-negative anaerobic bacteria usually found as part of the upper gastrointestinal and respiratory tract. They are an unusual cause of CAP but do occasionally occur, usually in middle-aged men with a history of recent high alcohol intake (presumably this means they aspirate some of their upper gastrointestinal tract bacteria because the overuse of alcohol prevents them from protecting their airway). The condition is known as
Necrobacillosis and presents as a particularly severe form of pneumonia requiring long courses of antibiotics such as Penicillin, Metronidazole or Clindamycin.
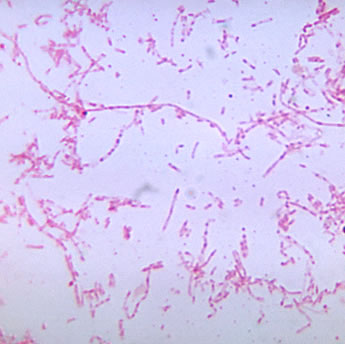
CDC image library: Dr. V. R. Dowell, Jr. Fusobacterium necrophorum in Gram film, showing the Gram-negative pleomorphic (variable shape) appearance of the organism
In this case the patient made a full recovery after 4 weeks of antibiotics. If your patient is not responding to treatment, it may not be the “spindly bacterium of death” but it is often worthwhile going back to the beginning and
re-examining the patient. Try to ignore your previous clerking and avoid a quick re-examination and assessment. Look afresh for new signs, symptoms and complications, which may not have been present on admission.
re-examining the patient. Try to ignore your previous clerking and avoid a quick re-examination and assessment. Look afresh for new signs, symptoms and complications, which may not have been present on admission.
 RSS Feed
RSS Feed
