My last blog was about the impending doom of the post-antibiotic era and one of the points raised by readers was “what about phages”? Well it’s such a good question that this is going to be the topic of this week’s blog!
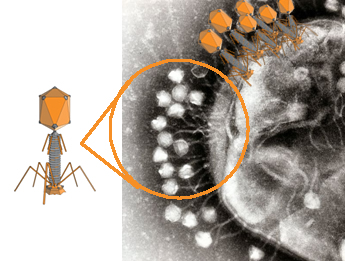
Bacteriophages, or “phages” as they are commonly known, are viruses that infect bacterial cells. They attach to the outside of bacterial cells and inject genes into the bacterium which causes lysis and destroys the infecting bacteria. To me they look a bit like the lunar module that NASA launched into space back in the 1960s.
Bacteriophages, or “phages” as they are commonly known, are viruses that infect bacterial cells. They attach to the outside of bacterial cells and inject genes into the bacterium which causes lysis and destroys the infecting bacteria. To me they look a bit like the lunar module that NASA launched into space back in the 1960s.
All very exciting in an era of post-antibiotics but it may surprise you to know that bacteriophages were actually discovered before antibiotics. So why didn’t they become “wonder drugs” like antibiotics? The history of bacteriophages is important in understanding why they never caught on.
A brief history of bacteriophages
Back in 1896 a British bacteriologist, Ernest Hankin, observed that there was something living in the waters of the Ganges River in India which limited the spread of cholera epidemics in that country. He didn’t know for certain what this substance was but he had found bacteriophages, so history can’t really credit him with the discovery.
It wasn’t until 1915 when another British Bacteriologist, Frederick Twort, suggested viruses were responsible for the phenomenon first described by Hankin. However due to the outbreak of World War I and financial difficulties he wasn’t able to pursue his experiments. It was finally a French-Canadian Microbiologist, Felix d’Herelle, who proved bacteriophages exist two years later. Officially the credit is given to both Twort and d’Herelle.
In fact d’Herelle accidently discovered bacteriophages whilst trying to produce a vaccine against bacterial dysentery. By producing bacterium-free filtrates from the stool of French soldiers during an outbreak of Shigella dysentery in Paris he observed that something in the filtrates was killing the bacteria on his agar plates. He thought this was a virus that was parasitizing the bacteria. Like all good Microbiologists he listened to his wife and she proposed the name bacteriophage from “bacteria” and “phagein” (the Greek for to eat or devour!).
The next step in d’Herelle's studies was to try and treat dysentery with his newly discovered bacteriophages. The study was conducted in 1919 in Paris after d’Herelle “proved” the safety of his bacteriophages by having himself and all of the clinical staff involved as the first to ingest the bacteriophage preparation the day before! You can almost hear the conversation the next day...“we survived the night so let’s give it to a patient” (wasn’t experimental medicine great in those days...for those that survived)! The preparation was then given to a 12 year old boy who was dying from dysentery and within a day he was much improved and a few days later he was cured. Further patients were successfully treated and d’Herelle was so convinced of his findings that he subsequently went on to treat thousands of patients with cholera and bubonic plague in India with various new bacteriophage preparations. Gosh, there seems there might be something exciting in this! However, d’Herelle is also historically criticised for failing to produce firm data about the efficacy of bacteriophages.
In fact d’Herelle was so convinced about his new treatment that he set up a commercial laboratory in Paris producing a number of different bacteriophage preparations...one of the predecessors of the worldwide brand L’Oreal! Commercial production continued to be carried out both in Europe and the USA until the 1940s. The discovery of antibiotics in the Western world effectively stopped all further research into bacteriophages (although if my memory serves me right we used to phage-type Staphylococcus aureus so maybe we haven’t completely forgotten what a bacteriophage is).
The research did continue in the Soviet Union, most notably from 1923 at the Eliava Institute in Tbilisi, Georgia. Giorgi Eliava, its founder, collaborated with d’Herelle to commercially produce bacteriophages for medical use. In fact d’Herelle was about to move permanently to Georgia when Eliava was arrested by Stalin’s secret police, announced an “Enemy of the People”, and executed… unsurprisingly d’Herelle never actually moved to Georgia.
However, the company still continues today producing tons of bacteriophage preparations that are used to treat thousands of patients with infections caused by Staphylococci, Pseudomonas spp., Proteus spp. and many cases of bacterial gastroenteritis. In 1957, another Soviet company, the Hirszfield Institute, also began producing bacteriophages for treating septicaemia, skin infections and UTIs as well as infections caused by antibiotic-resistant bacteria. There have also been a number of studies from Poland where bacteriophages have been used to treat everything from meningitis in neonates, skin infections caused by Staphylococcus aureus, burns infected with Pseudomonas aeruginosa, gastrointestinal infections and even intra-abdominal abscesses.
So why did the West overlook bacteriophages? Because most of the literature was, and still is, in Russian! The West quite literally could not access it and even if they spoke Russian, who in the midst of the Cold War would admit to close ties with Russia?
Another major stumbling block against the acceptance of bacteriophages into clinical medicine in the West is the lack of blinded, randomised, controlled trials into their safety and efficacy. Although numerous studies “show” safe and effective use of bacteriophages almost invariably the studies are poorly designed and lacked a control group. Often patients were selected based on the criteria that they had already failed conventional antibiotic therapy, so maybe the lack of a control group can be forgiven because withholding a potential treatment could be considered unethical. However, we can accept the research findings that there were no side-effects with bacteriophage therapy, irrespective of whether there is a control group or not.
So how do bacteriophages work?
Here we hit another problem with why bacteriophages haven’t been accepted in to standard anti-infective therapy… no one really knows exactly how they work. But then no one really knows how Nitrofurantoin works either and yet it is given to millions of people every year for the treatment of UTIs. So surely how bacteriophages work is irrelevant as long as they do work!
What we do know is that bacteriophages invade bacterial cells and replicate inside those the cells. The presence of bacteriophages inside the bacterial cell causes a cascade of events which damages structural and regulatory genes causing the bacteria to lyse. However, this cascade has not been fully determined and not all bacteriophages behave in the same way. We also know that bacteriophages reproduce in the bacterial cells at the site of the infection; therefore the ongoing infection actually helps increase the number of bacteriophages by providing the environment for the bacteriophages to replicate in. This continued replication can allow infrequent dosing of bacteriophages to be used. Once the bacteria are destroyed the bacteriophages no longer have something to replicate in and therefore their numbers fall away rapidly.
A brief history of bacteriophages
Back in 1896 a British bacteriologist, Ernest Hankin, observed that there was something living in the waters of the Ganges River in India which limited the spread of cholera epidemics in that country. He didn’t know for certain what this substance was but he had found bacteriophages, so history can’t really credit him with the discovery.
It wasn’t until 1915 when another British Bacteriologist, Frederick Twort, suggested viruses were responsible for the phenomenon first described by Hankin. However due to the outbreak of World War I and financial difficulties he wasn’t able to pursue his experiments. It was finally a French-Canadian Microbiologist, Felix d’Herelle, who proved bacteriophages exist two years later. Officially the credit is given to both Twort and d’Herelle.
In fact d’Herelle accidently discovered bacteriophages whilst trying to produce a vaccine against bacterial dysentery. By producing bacterium-free filtrates from the stool of French soldiers during an outbreak of Shigella dysentery in Paris he observed that something in the filtrates was killing the bacteria on his agar plates. He thought this was a virus that was parasitizing the bacteria. Like all good Microbiologists he listened to his wife and she proposed the name bacteriophage from “bacteria” and “phagein” (the Greek for to eat or devour!).
The next step in d’Herelle's studies was to try and treat dysentery with his newly discovered bacteriophages. The study was conducted in 1919 in Paris after d’Herelle “proved” the safety of his bacteriophages by having himself and all of the clinical staff involved as the first to ingest the bacteriophage preparation the day before! You can almost hear the conversation the next day...“we survived the night so let’s give it to a patient” (wasn’t experimental medicine great in those days...for those that survived)! The preparation was then given to a 12 year old boy who was dying from dysentery and within a day he was much improved and a few days later he was cured. Further patients were successfully treated and d’Herelle was so convinced of his findings that he subsequently went on to treat thousands of patients with cholera and bubonic plague in India with various new bacteriophage preparations. Gosh, there seems there might be something exciting in this! However, d’Herelle is also historically criticised for failing to produce firm data about the efficacy of bacteriophages.
In fact d’Herelle was so convinced about his new treatment that he set up a commercial laboratory in Paris producing a number of different bacteriophage preparations...one of the predecessors of the worldwide brand L’Oreal! Commercial production continued to be carried out both in Europe and the USA until the 1940s. The discovery of antibiotics in the Western world effectively stopped all further research into bacteriophages (although if my memory serves me right we used to phage-type Staphylococcus aureus so maybe we haven’t completely forgotten what a bacteriophage is).
The research did continue in the Soviet Union, most notably from 1923 at the Eliava Institute in Tbilisi, Georgia. Giorgi Eliava, its founder, collaborated with d’Herelle to commercially produce bacteriophages for medical use. In fact d’Herelle was about to move permanently to Georgia when Eliava was arrested by Stalin’s secret police, announced an “Enemy of the People”, and executed… unsurprisingly d’Herelle never actually moved to Georgia.
However, the company still continues today producing tons of bacteriophage preparations that are used to treat thousands of patients with infections caused by Staphylococci, Pseudomonas spp., Proteus spp. and many cases of bacterial gastroenteritis. In 1957, another Soviet company, the Hirszfield Institute, also began producing bacteriophages for treating septicaemia, skin infections and UTIs as well as infections caused by antibiotic-resistant bacteria. There have also been a number of studies from Poland where bacteriophages have been used to treat everything from meningitis in neonates, skin infections caused by Staphylococcus aureus, burns infected with Pseudomonas aeruginosa, gastrointestinal infections and even intra-abdominal abscesses.
So why did the West overlook bacteriophages? Because most of the literature was, and still is, in Russian! The West quite literally could not access it and even if they spoke Russian, who in the midst of the Cold War would admit to close ties with Russia?
Another major stumbling block against the acceptance of bacteriophages into clinical medicine in the West is the lack of blinded, randomised, controlled trials into their safety and efficacy. Although numerous studies “show” safe and effective use of bacteriophages almost invariably the studies are poorly designed and lacked a control group. Often patients were selected based on the criteria that they had already failed conventional antibiotic therapy, so maybe the lack of a control group can be forgiven because withholding a potential treatment could be considered unethical. However, we can accept the research findings that there were no side-effects with bacteriophage therapy, irrespective of whether there is a control group or not.
So how do bacteriophages work?
Here we hit another problem with why bacteriophages haven’t been accepted in to standard anti-infective therapy… no one really knows exactly how they work. But then no one really knows how Nitrofurantoin works either and yet it is given to millions of people every year for the treatment of UTIs. So surely how bacteriophages work is irrelevant as long as they do work!
What we do know is that bacteriophages invade bacterial cells and replicate inside those the cells. The presence of bacteriophages inside the bacterial cell causes a cascade of events which damages structural and regulatory genes causing the bacteria to lyse. However, this cascade has not been fully determined and not all bacteriophages behave in the same way. We also know that bacteriophages reproduce in the bacterial cells at the site of the infection; therefore the ongoing infection actually helps increase the number of bacteriophages by providing the environment for the bacteriophages to replicate in. This continued replication can allow infrequent dosing of bacteriophages to be used. Once the bacteria are destroyed the bacteriophages no longer have something to replicate in and therefore their numbers fall away rapidly.

Click for larger image
I can see the day when clinical treatment might be a standard vial of anti-Staphylococcal bacteriophages for empirical treatment of cellulitis or anti-Enterobacteriaceae bacteriophages for empirical treatment of UTIs. Once the specific cause has been identified in the laboratory the most effective and specific bacteriophage can be determined for ongoing treatment. So bacteriophages are basically highly specific, benefit from infrequent dosing, no side-effects and once no longer required to fight the infection they breakdown and disappear meaning less chance of causing an adverse effect. They sound really great don’t they?!
But are they really safe?
Intuitively bacteriophages should be safe, as they attack bacteria not human cells, and studies suggest this is the case. Bacteriophages are common in our environment with reports suggesting that even non-polluted water contains 200 million bacteriophages per ml of water and they live in the bacteria on food so they are regularly consumed every day. Bacteriophages have therefore evolved with humans and we appear to have adapted to their presence without them causing us harm.
Summary of bacteriophage therapy
There are a number of proposed advantages to bacteriophage therapy:
However, there are a number of problems and concerns limiting the research and development of bacteriophage therapy:
So what is my opinion?
I think that “absence of evidence doesn’t mean evidence of absence”. Given that no one has proven that they don’t work, and we are out of time with antibiotics, let’s give bacteriophages a chance. Let the thorough examination begin: definitively establish if they do work, prove that they are safe, develop methods of testing them within the existing laboratory service and integrate this new treatment and into the Western medical system. Who knows, maybe the “post-antibiotic era” will become the “bacteriophage era”?
But are they really safe?
Intuitively bacteriophages should be safe, as they attack bacteria not human cells, and studies suggest this is the case. Bacteriophages are common in our environment with reports suggesting that even non-polluted water contains 200 million bacteriophages per ml of water and they live in the bacteria on food so they are regularly consumed every day. Bacteriophages have therefore evolved with humans and we appear to have adapted to their presence without them causing us harm.
Summary of bacteriophage therapy
There are a number of proposed advantages to bacteriophage therapy:
- They are specific to bacterial species level therefore collateral damage to the rest of our normal flora is limited
- They replicate at the site of infection and therefore naturally increase their levels where they are most needed
- No serious complications have been described
- If a bacterium is resistant to a specific bacteriophage it is usually still susceptible to other bacteriophages
- Selecting new phages to treat specific bacteria is relatively cheap and quick taking only a matter of a few days
However, there are a number of problems and concerns limiting the research and development of bacteriophage therapy:
- Concerns about the purity of bacteriophage preparations which may contain other bacteria and toxins which could adversely affect patients
- The limited “shelf life” of bacteriophages which means that unless used rapidly after production the bacteriophages may actually have become inactive
- Inadequate understanding of the modes of actions of bacteriophages
- Poor quality historical research which does not meet the body of proof required by modern standards (NB: Although I suspect this same argument could be applied to many antibiotics if we really wanted to be picky about it!)
So what is my opinion?
I think that “absence of evidence doesn’t mean evidence of absence”. Given that no one has proven that they don’t work, and we are out of time with antibiotics, let’s give bacteriophages a chance. Let the thorough examination begin: definitively establish if they do work, prove that they are safe, develop methods of testing them within the existing laboratory service and integrate this new treatment and into the Western medical system. Who knows, maybe the “post-antibiotic era” will become the “bacteriophage era”?
 RSS Feed
RSS Feed
