The patient this week was admitted with cellulitis of her lower leg which was not getting better with oral Flucloxacillin from her GP. She had been switched from oral Flucloxacillin to IV by the ward doctors and after 3 days her cellulitis had progressed to involve her entire leg. The doctors questioned whether the patient might have a resistant bacteria e.g. Meticillin Resistant Staphylococcus aureus (MRSA) and switched the patient to Teicoplanin at the “normal doses” in the BNF. A further 48 hours later she was no better and they phoned the Microbiologist for advice.
So what is the first question I asked in this scenario; other than has the antimicrobial actually been given?!? It’s “Do you need to supersize that antibiotic?”
So what is the first question I asked in this scenario; other than has the antimicrobial actually been given?!? It’s “Do you need to supersize that antibiotic?”
... I mean “how much does the patient weigh?” Almost every time the patient is morbidly obese and that is the reason they are not getting better. Supersize is a phrase coined by McDonald’s to sizably increase their French fries and soft drinks to an extra-large size. Although McDonald's phased out the supersized option in 2001 (stating the need to simplify their menu rather than concerns over obesity lawsuits) globally body weight has continued to supersize and obesity is now effecting how we prescribe. If you want to keep a figure in your head about when an average height patient becomes morbidly obese it’s 105kg for women and 125kg for men… I bet if you look around the wards or in clinic you’ll see patients who fall into this group.
I believe the problem is growing so large that I am changing the way I teach antimicrobials. I used to make sure students remembered that for certain key infections there are different antimicrobial doses compared to those normally used. For example: meningitis should be treated with 2g BD of Ceftriaxone whereas for most other infections the treatment dose is 1g OD, or infective endocarditis should be treated with 2g 4 hourly of Amoxicillin whereas most other infections require just 1g TDS. But now I add morbid obesity to these exceptions, I find myself telling doctors and pharmacists that the correct antimicrobial dose ALSO has to take into account the weight of the patient!
When I am on duty I have at least 5 calls per week where I have to give antimicrobial dosing advice for patients who are morbidly obese (BMI >40) and although infrequent, I have even had to come up with antimicrobial regimens for patients who weigh more than 250kg, i.e. BMI 80-100 kg/m2. This is 3-4 times the medically accepted “normal” body weight…so what has changed since I went to medical school in 1992 and how is it effecting practise? The most obvious change is the number of obese patients we have to manage in the NHS...the effect, well...
The Worldwide Obesity Epidemic
According to the World Health Organisation we are in the middle of a global obesity epidemic. Obesity is defined as a Body Mass Index of >30kg/m2. In the UK the incidence of obesity in adults has increased from 14.9% in 1993 to 24.9% in 2013… That’s 10% in only 20 years. The number of adults overweight or obese (BMI >25 kg/m2) is now 62.1%... yes that’s nearly two thirds of the adult population! Morbid obesity (BMI >40 kg/m2) is said to be around 4% for women and 2% for men in 2013 whereas it was virtually non-existent in 1993. These are terrifying statistics!
I now find myself questioning comments from doctors phoning for advice who tell me their patient is a “normal” weight. What is normal? The comment “normal” means that they sit within the centre of a normally distributed value (remember your days of doing statistics at school and that funny hill of a curve on a graph). Normal weight is 60-70kg body weight (BMI 20-25 kg/m2). But as two thirds of the adult population is now overweight I suspect the normal distribution has also shifted. Therefore today’s “normal” now means overweight. So does the doctor calling me mean their patient is overweight and normal for today’s population or of a healthy weight which is in fact not “normal” for today’s population? Doctors should hold onto the idea that if 62.1% of the population is overweight or obese this is very “abnormal”.
I’m dealing with the issue around antimicrobial dosing in morbid obesity because it has an impact on my work every day.
Why are antimicrobial doses inadequate in morbidly obese patients?
The most obvious reason why antimicrobial doses are inadequate in morbidly obese patients is that there is just a lot more patient to treat and the volume of body in which the antimicrobial is spread out is much greater. This would be less of a problem for antimicrobials if they stayed in the blood stream and only entered body tissues which were infected but this is clearly not the case. Antimicrobials distribute to different types of tissue in different amounts. Lipid bound antimicrobials are going to be seriously reduced in obese patients who have large amounts of body lipid to bind the antimicrobial. This is especially the case with antimicrobials like the glycopeptides, lipopeptides and the polyenes.
There is another reason why antimicrobial doses are often inadequate in obese patients; the doses were all worked out before obesity was a common problem. Most antimicrobials were discovered before 1960 with the doses based upon research done in the 1940s and 1950s; an era when “normal” did equate to a “healthy” 60-70kg body weight. In the 1960s patients weighed considerably less than they do now, almost no one then had a BMI >40 kg/m2, and obesity was much less common due in part to an era of rationing, post-World War II austerity and more daily activity (in the 1960s the percentage overweight in the USA was around 30% while in the UK it was only 1-2%).
What effect does obesity have on infection and antimicrobial prescribing?
So what dose of antimicrobials should we use?
The doses we have are just not up to the task but we have little research or evidence to help us decide on appropriate doses for our morbidly obese patients.
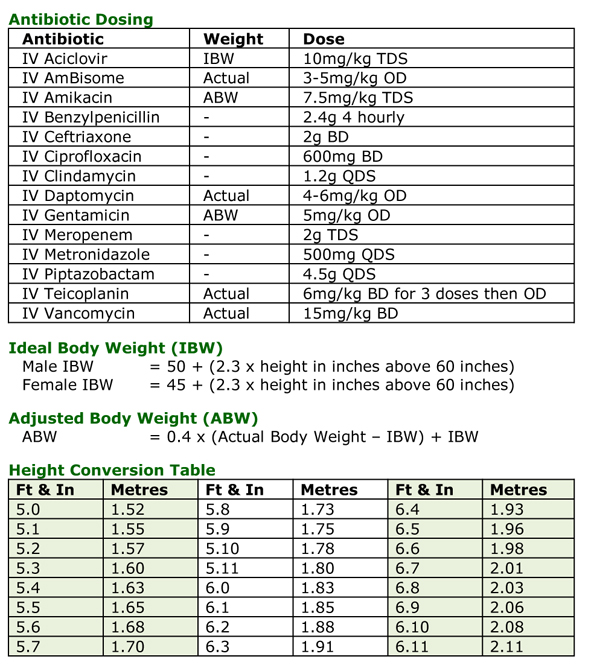
There are only 7 antimicrobials where we do know how to adjust the dose in morbid obesity: Aciclovir, AmBisome, Amikacin, Daptomycin, Gentamicin, Teicoplanin and Vancomycin. For all other antimicrobials I tend to use the highest dose allowed in the BNF or product literature. The following table is the dosing I use in morbidly obese patients when I am giving advice.
When I am on duty I have at least 5 calls per week where I have to give antimicrobial dosing advice for patients who are morbidly obese (BMI >40) and although infrequent, I have even had to come up with antimicrobial regimens for patients who weigh more than 250kg, i.e. BMI 80-100 kg/m2. This is 3-4 times the medically accepted “normal” body weight…so what has changed since I went to medical school in 1992 and how is it effecting practise? The most obvious change is the number of obese patients we have to manage in the NHS...the effect, well...
The Worldwide Obesity Epidemic
According to the World Health Organisation we are in the middle of a global obesity epidemic. Obesity is defined as a Body Mass Index of >30kg/m2. In the UK the incidence of obesity in adults has increased from 14.9% in 1993 to 24.9% in 2013… That’s 10% in only 20 years. The number of adults overweight or obese (BMI >25 kg/m2) is now 62.1%... yes that’s nearly two thirds of the adult population! Morbid obesity (BMI >40 kg/m2) is said to be around 4% for women and 2% for men in 2013 whereas it was virtually non-existent in 1993. These are terrifying statistics!
I now find myself questioning comments from doctors phoning for advice who tell me their patient is a “normal” weight. What is normal? The comment “normal” means that they sit within the centre of a normally distributed value (remember your days of doing statistics at school and that funny hill of a curve on a graph). Normal weight is 60-70kg body weight (BMI 20-25 kg/m2). But as two thirds of the adult population is now overweight I suspect the normal distribution has also shifted. Therefore today’s “normal” now means overweight. So does the doctor calling me mean their patient is overweight and normal for today’s population or of a healthy weight which is in fact not “normal” for today’s population? Doctors should hold onto the idea that if 62.1% of the population is overweight or obese this is very “abnormal”.
I’m dealing with the issue around antimicrobial dosing in morbid obesity because it has an impact on my work every day.
Why are antimicrobial doses inadequate in morbidly obese patients?
The most obvious reason why antimicrobial doses are inadequate in morbidly obese patients is that there is just a lot more patient to treat and the volume of body in which the antimicrobial is spread out is much greater. This would be less of a problem for antimicrobials if they stayed in the blood stream and only entered body tissues which were infected but this is clearly not the case. Antimicrobials distribute to different types of tissue in different amounts. Lipid bound antimicrobials are going to be seriously reduced in obese patients who have large amounts of body lipid to bind the antimicrobial. This is especially the case with antimicrobials like the glycopeptides, lipopeptides and the polyenes.
There is another reason why antimicrobial doses are often inadequate in obese patients; the doses were all worked out before obesity was a common problem. Most antimicrobials were discovered before 1960 with the doses based upon research done in the 1940s and 1950s; an era when “normal” did equate to a “healthy” 60-70kg body weight. In the 1960s patients weighed considerably less than they do now, almost no one then had a BMI >40 kg/m2, and obesity was much less common due in part to an era of rationing, post-World War II austerity and more daily activity (in the 1960s the percentage overweight in the USA was around 30% while in the UK it was only 1-2%).
What effect does obesity have on infection and antimicrobial prescribing?
- Increased susceptibility to infection, especially wound infections irrespective of the associated increased risk as a result of type 2 diabetes mellitus in this group of patients
- Increased complications from infections, especially respiratory complications related to lower respiratory tract infections
- Possible immune deficiency related to low levels of leptin, but whilst the observation of immune deficiency is real the cause is yet to be proven
- Larger doses of antimicrobials cost the NHS more money, let alone longer patient stays in hospital
- Unknown antimicrobial dosing requirements to treat even common infections
- Low systemic levels of antimicrobials are likely to promote the selection of antimicrobial resistant bacteria
So what dose of antimicrobials should we use?
The doses we have are just not up to the task but we have little research or evidence to help us decide on appropriate doses for our morbidly obese patients.
There are only 7 antimicrobials where we do know how to adjust the dose in morbid obesity: Aciclovir, AmBisome, Amikacin, Daptomycin, Gentamicin, Teicoplanin and Vancomycin. For all other antimicrobials I tend to use the highest dose allowed in the BNF or product literature. The following table is the dosing I use in morbidly obese patients when I am giving advice.
Click for larger image
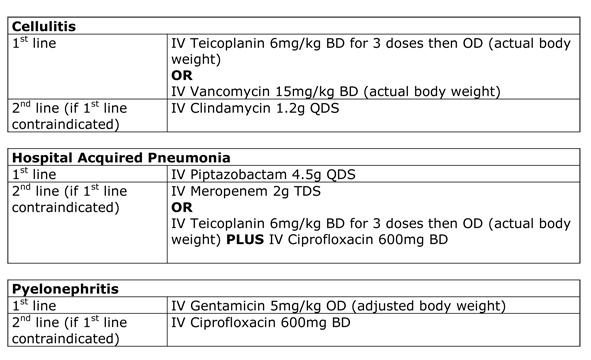
The 3 most common clinical scenarios where I find myself giving advice are cellulitis, hospital acquired pneumonia and pyelonephritis. The following are my recommendations for morbidly obese patients in these scenarios:
Click for larger image
So what can you do for your patients?
Firstly always treat the patient with an antimicrobial that you know will treat their current infection; then consider a dose appropriate for a morbidly obese patient. If the patient doesn’t improve it is a good idea to get the advice of a Microbiologist or Infectious Diseases Physician who may be able to come up with other antimicrobial regimens to treat the patient.
I think it’s also important to make patients aware of the impact their weight has on their management. They need to be told that antibiotic doses are based upon patients who weighed 60-70kg (not 105-125kg or more) and that we as doctors don’t really know what dose to use to treat morbidly obese patients. The discussion should also include making the patient aware that as a result of their weight they may not get better with the antimicrobial regimens being tried and that this is not the result of a poor choice of antimicrobial; the doctor is using the most effective treatment they can. It is not about being unkind; it’s about making the patient fully aware of the difficulties and problems that their weight causes to their medical treatment. One of the problems we face is that as obesity becomes more and more prevalent, the population becomes less inclined to get back to a normal weight – the population has been supersized and the social norm has shifted. So do you think you should be supersizing any of your patient’s antibiotics?
Firstly always treat the patient with an antimicrobial that you know will treat their current infection; then consider a dose appropriate for a morbidly obese patient. If the patient doesn’t improve it is a good idea to get the advice of a Microbiologist or Infectious Diseases Physician who may be able to come up with other antimicrobial regimens to treat the patient.
I think it’s also important to make patients aware of the impact their weight has on their management. They need to be told that antibiotic doses are based upon patients who weighed 60-70kg (not 105-125kg or more) and that we as doctors don’t really know what dose to use to treat morbidly obese patients. The discussion should also include making the patient aware that as a result of their weight they may not get better with the antimicrobial regimens being tried and that this is not the result of a poor choice of antimicrobial; the doctor is using the most effective treatment they can. It is not about being unkind; it’s about making the patient fully aware of the difficulties and problems that their weight causes to their medical treatment. One of the problems we face is that as obesity becomes more and more prevalent, the population becomes less inclined to get back to a normal weight – the population has been supersized and the social norm has shifted. So do you think you should be supersizing any of your patient’s antibiotics?
 RSS Feed
RSS Feed
