“We have a young child with a fever and a rash who isn’t very well and we want to test for measles” said the Junior Doctor working in Paediatrics.
“Have they been vaccinated?” asked the Microbiologist in reply.
“No, their Mum was worried about the vaccine and so they haven’t had it done” was the response.
“Do they have any spots in their mouth?” asked the Microbiologist.
“They don’t have any spots, it’s not Chicken Pox it’s more like measles…” replied the Doctor sounding confused.
“They’re called Koplik spots, maybe get a Consultant to have a look. Is the child isolated?”
“Errrmmmm…” replied the Doctor “I don’t think so…”
“Have they been vaccinated?” asked the Microbiologist in reply.
“No, their Mum was worried about the vaccine and so they haven’t had it done” was the response.
“Do they have any spots in their mouth?” asked the Microbiologist.
“They don’t have any spots, it’s not Chicken Pox it’s more like measles…” replied the Doctor sounding confused.
“They’re called Koplik spots, maybe get a Consultant to have a look. Is the child isolated?”
“Errrmmmm…” replied the Doctor “I don’t think so…”
“Damn! Measles is highly infectious. Get the child isolated, look in the mouth, and I’ll arrange for a diagnostic kit. I’ll also need to start the infection control process rolling in case you have exposed anyone to measles…” the Microbiologist exclaimed.
After hanging up the Microbiologist popped his head into the infection control team’s office… ”you’re not going to be happy about this one…!” he said with a grimace on his face.
What is measles?
So almost everyone these days knows that measles is a viral infection that causes a fever and a rash… or is it?
The Measles Virus is part of the Paramyxoviridae family which is part of the larger group of Morbilliviruses. In fact the rash caused by measles is called a morbilliform rash, and any rash that looks the same is given the same name; the rash is red and macular (not raised and cannot be felt) and usually 2–10 mm in diameter but may be confluent in places.
In 2018 in Europe, there were more than 82,500 cases, three times more than 2017. Measles has a mortality of 1 in 1000 cases and in 2017 there were 110,000 deaths Worldwide. The myth that measles is a trivial febrile rash illness is wrong; measles can kill. Any death from measles is a tragedy since measles is a preventable disease.
So far in the UK this year there have been over 800 cases, this means we will likely have over 2,000 cases in 2019 and therefore more than 2 children in the UK are likely to die from measles. However, there is currently a media storm around the USA having multiple measles outbreaks and yet there have only been 626 cases in the USA so far in 2019 from a population much larger than the UK. Am I the only person concerned about the rates of measles in the UK?
How does measles present?
Patients with measles usually have a prodromal period of high fever, cough, conjunctivitis and “cold-like” symptoms for two days prior to a rash appearing.
The rash typically appears first behind the ears and then spreads down the body; usually the severity of the rash corresponds to the severity of the illness. Most patients in the prodromal period develop bluish-white spots inside their cheeks (buccal mucosa) known as Koplik spots, which are diagnostic of measles.
Patients usually begin to improve 3 days after the rash appears and the majority are back to normal after 7-10 days.
Complications occur in 6-7% of patients and include:
*Pneumonitis and encephalitis are the most common causes of death in measles.
The most feared complication of measles is the “ticking time bomb” Subacute Sclerosing Panencephalitis (SSPE) … it occurs 5-10 years after the initial infection and cannot be predicted. It is thought to be due to chronic measles infection in the central nervous system. SSPE occurs in 5-10 per 100,000 cases overall but 18 per 100,000 where measles occurred in infancy. SSPE presents with gradual neurological symptoms such as personality change, lethargy and altered behaviour. This worsens over the next few years eventually leading to the onset of severe myoclonic jerks every 5-10 seconds, dementia and motor and sensory neurological disturbance, which can last up to 12 months. Finally the patient develops a persistent vegetative state with either flaccid or rigid paralysis. Death is inevitable.
I have looked after a patient with SSPE and it was awful for the patient, their family and the healthcare team. The patient had not been vaccinated.
How is measles diagnosed?
In the UK measles is diagnosed using a buccal swab to collect saliva. The swab looks like a small bit of sponge on a plastic lolly stick, similar to those used to wet patient’s mouths with water when they are not allowed to drink (please don’t send these as swabs!). The swab kit is acquired directly from Public Health England and the sample is sent directly to the Reference Laboratory at Colindale, London, who test for measles IgM. They can also test for the virus itself by PCR if needed for epidemiological purposes. A positive measles IgM confirms the diagnosis.
How is measles treated?
There is no specific antiviral for measles; supportive care with fluids, antipyretics and oxygen as required are the mainstays of treatment. The WHO recommend giving all patients with measles a course of Vitamin A as deficiency of this vitamin is associated with severe infection and higher mortality.
How is measles spread?
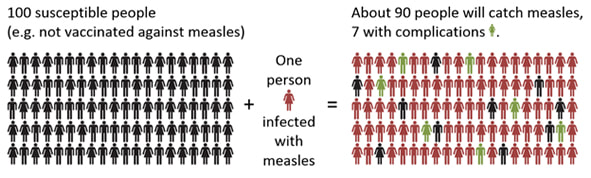
Measles is spread via droplets from the upper respiratory tract. It is one of the most infectious viruses. It is estimated that every single person with measles infects 90 others; this is because 90% of susceptible people exposed to measles develop infection. Measles Virus can survive for about 2 hours on surfaces and as well as remain suspended as aerosolized particles for a few hours. Given that people are infectious for 48 hours before the rash appears and until 4-5 days after, is easy to see how people can be infected without even knowing they have been exposed… if measles is circulating in a community you cannot avoid it!
After hanging up the Microbiologist popped his head into the infection control team’s office… ”you’re not going to be happy about this one…!” he said with a grimace on his face.
What is measles?
So almost everyone these days knows that measles is a viral infection that causes a fever and a rash… or is it?
The Measles Virus is part of the Paramyxoviridae family which is part of the larger group of Morbilliviruses. In fact the rash caused by measles is called a morbilliform rash, and any rash that looks the same is given the same name; the rash is red and macular (not raised and cannot be felt) and usually 2–10 mm in diameter but may be confluent in places.
In 2018 in Europe, there were more than 82,500 cases, three times more than 2017. Measles has a mortality of 1 in 1000 cases and in 2017 there were 110,000 deaths Worldwide. The myth that measles is a trivial febrile rash illness is wrong; measles can kill. Any death from measles is a tragedy since measles is a preventable disease.
So far in the UK this year there have been over 800 cases, this means we will likely have over 2,000 cases in 2019 and therefore more than 2 children in the UK are likely to die from measles. However, there is currently a media storm around the USA having multiple measles outbreaks and yet there have only been 626 cases in the USA so far in 2019 from a population much larger than the UK. Am I the only person concerned about the rates of measles in the UK?
How does measles present?
Patients with measles usually have a prodromal period of high fever, cough, conjunctivitis and “cold-like” symptoms for two days prior to a rash appearing.
The rash typically appears first behind the ears and then spreads down the body; usually the severity of the rash corresponds to the severity of the illness. Most patients in the prodromal period develop bluish-white spots inside their cheeks (buccal mucosa) known as Koplik spots, which are diagnostic of measles.
Patients usually begin to improve 3 days after the rash appears and the majority are back to normal after 7-10 days.
Complications occur in 6-7% of patients and include:
- Diarrhoea (80 in 1,000)
- Otitis media (50 in 1,000)
- Pneumonitis (38 in 1,000)*
- Convulsions (5 in 1,000)
- Encephalitis (1.2 in 1,000)*
- Idiopathic thrombocytopaenic purpura (1 in 2,000)
*Pneumonitis and encephalitis are the most common causes of death in measles.
The most feared complication of measles is the “ticking time bomb” Subacute Sclerosing Panencephalitis (SSPE) … it occurs 5-10 years after the initial infection and cannot be predicted. It is thought to be due to chronic measles infection in the central nervous system. SSPE occurs in 5-10 per 100,000 cases overall but 18 per 100,000 where measles occurred in infancy. SSPE presents with gradual neurological symptoms such as personality change, lethargy and altered behaviour. This worsens over the next few years eventually leading to the onset of severe myoclonic jerks every 5-10 seconds, dementia and motor and sensory neurological disturbance, which can last up to 12 months. Finally the patient develops a persistent vegetative state with either flaccid or rigid paralysis. Death is inevitable.
I have looked after a patient with SSPE and it was awful for the patient, their family and the healthcare team. The patient had not been vaccinated.
How is measles diagnosed?
In the UK measles is diagnosed using a buccal swab to collect saliva. The swab looks like a small bit of sponge on a plastic lolly stick, similar to those used to wet patient’s mouths with water when they are not allowed to drink (please don’t send these as swabs!). The swab kit is acquired directly from Public Health England and the sample is sent directly to the Reference Laboratory at Colindale, London, who test for measles IgM. They can also test for the virus itself by PCR if needed for epidemiological purposes. A positive measles IgM confirms the diagnosis.
How is measles treated?
There is no specific antiviral for measles; supportive care with fluids, antipyretics and oxygen as required are the mainstays of treatment. The WHO recommend giving all patients with measles a course of Vitamin A as deficiency of this vitamin is associated with severe infection and higher mortality.
How is measles spread?
Measles is spread via droplets from the upper respiratory tract. It is one of the most infectious viruses. It is estimated that every single person with measles infects 90 others; this is because 90% of susceptible people exposed to measles develop infection. Measles Virus can survive for about 2 hours on surfaces and as well as remain suspended as aerosolized particles for a few hours. Given that people are infectious for 48 hours before the rash appears and until 4-5 days after, is easy to see how people can be infected without even knowing they have been exposed… if measles is circulating in a community you cannot avoid it!
Click for larger image
I thought measles was only of historical interest, why is it back?
Cases of measles are on the climb because vaccination rates are falling. In order to prevent measles from circulating within a community you need to reach a high level of “herd immunity” i.e. enough people are immunised to protect those that aren’t. The rate of immunisation to protect from measles is 95% of the population.
In the UK the current rate of immunisation with a single dose of vaccine is 92% and the recommended 2 doses is even lower, 87%. This is well below the level needed to prevent measles from circulating and there are now over 500,000 children who are not immune to measles. Some areas do particularly poorly; none of the 32 London authorities have made the 95% target in the last 5 years (2013-2018). Some London boroughs consistently have rates radically lower including Hackney and City of London (75%), Westminster (77.5%) and Kensington and Chelsea (78%). Westminster saw its rate fall as low as 69.3% in 2016-2017! Out of the 30 local authorities in the South East and East England only 1 made the 95% target. Why is that? Well…in 1998 the Lancet published (and has since retracted) the research paper by Wakefield that sparked the MMR scare; this, along with the unbalanced media coverage that followed, saw average UK vaccination rates fall to as low as only 80% in 2004. Rates are still not back up to the pre-scandal levels. If you want to know how your area is doing, then have a look at this interactive map (click to slide 3, it's the most fun!).
Those low levels of immunisation are now coming back to haunt us with all of those adolescents and young adults who should have been vaccinated in the early 2000s not actually being immune to measles.
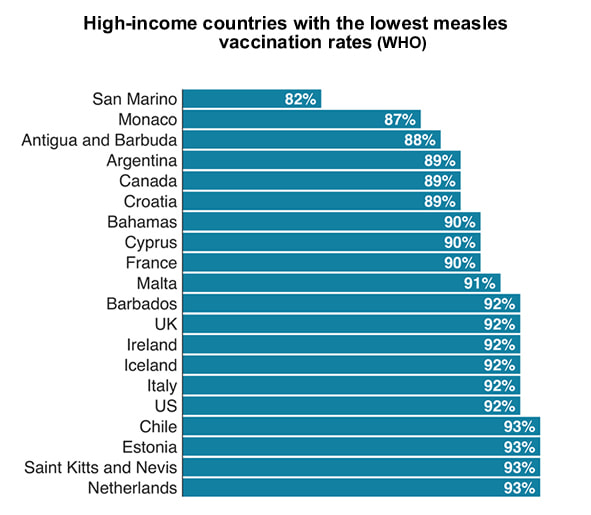
The situation is bad in high-income countries but in fact vaccination rates worldwide are well below the required 95% target set by the WHO to gain herd immunity. Only raising global vaccination rates will actually eradicate measles, a task which is possible as humans are the only carriers of the virus. If you returned to the 1800s and told the population of London that with a vaccination measles could be eradicated, I wonder if they would have the injection?
Cases of measles are on the climb because vaccination rates are falling. In order to prevent measles from circulating within a community you need to reach a high level of “herd immunity” i.e. enough people are immunised to protect those that aren’t. The rate of immunisation to protect from measles is 95% of the population.
In the UK the current rate of immunisation with a single dose of vaccine is 92% and the recommended 2 doses is even lower, 87%. This is well below the level needed to prevent measles from circulating and there are now over 500,000 children who are not immune to measles. Some areas do particularly poorly; none of the 32 London authorities have made the 95% target in the last 5 years (2013-2018). Some London boroughs consistently have rates radically lower including Hackney and City of London (75%), Westminster (77.5%) and Kensington and Chelsea (78%). Westminster saw its rate fall as low as 69.3% in 2016-2017! Out of the 30 local authorities in the South East and East England only 1 made the 95% target. Why is that? Well…in 1998 the Lancet published (and has since retracted) the research paper by Wakefield that sparked the MMR scare; this, along with the unbalanced media coverage that followed, saw average UK vaccination rates fall to as low as only 80% in 2004. Rates are still not back up to the pre-scandal levels. If you want to know how your area is doing, then have a look at this interactive map (click to slide 3, it's the most fun!).
Those low levels of immunisation are now coming back to haunt us with all of those adolescents and young adults who should have been vaccinated in the early 2000s not actually being immune to measles.
The situation is bad in high-income countries but in fact vaccination rates worldwide are well below the required 95% target set by the WHO to gain herd immunity. Only raising global vaccination rates will actually eradicate measles, a task which is possible as humans are the only carriers of the virus. If you returned to the 1800s and told the population of London that with a vaccination measles could be eradicated, I wonder if they would have the injection?
Click for larger image
Controlling outbreaks?
In the USA there have been 626 measles cases across 22 states in 2019, even though the USA declared measles eradicated in 2000! Technically in the USA all 50 states have laws requiring children attending public school to be vaccinated, but 17 allow exception for “personal philosophical exceptions”. New York State is taking extreme measures to try and control their measles outbreak; children less than 18 years old who have not been vaccinated are being banned from public places and anyone who breaks this rule faces a fine and 6 months in prison!
In the UK the Health and Social Care Secretary, Matt Hancock, has called for new legislation to force social media companies to remove content promoting false information about vaccines. Whether this is feasible waits to be seen but it might help. Maybe responsible reporting from mainstream media like the BBC and ITN would also be helpful as they helped fuel the Wakefield debacle, yet now criticise vaccination uptake!?
...A little while after having spoken to the Paediatric Junior Doctor the Consultant Paediatrician rang the Microbiologist back. The child did indeed have Koplik spots and was now in a side room. The Paediatrician was very apologetic but had spoken to the other parents in the same area as the patient about vaccination history, whilst being careful not to breach confidentiality, and had ascertained that all the other patients and parents were immune. A list of staff had been drawn up and the ward Matron was this very minute talking to Occupational Health… at least the response after the diagnosis was excellent thought the Microbiologist….
In the USA there have been 626 measles cases across 22 states in 2019, even though the USA declared measles eradicated in 2000! Technically in the USA all 50 states have laws requiring children attending public school to be vaccinated, but 17 allow exception for “personal philosophical exceptions”. New York State is taking extreme measures to try and control their measles outbreak; children less than 18 years old who have not been vaccinated are being banned from public places and anyone who breaks this rule faces a fine and 6 months in prison!
In the UK the Health and Social Care Secretary, Matt Hancock, has called for new legislation to force social media companies to remove content promoting false information about vaccines. Whether this is feasible waits to be seen but it might help. Maybe responsible reporting from mainstream media like the BBC and ITN would also be helpful as they helped fuel the Wakefield debacle, yet now criticise vaccination uptake!?
...A little while after having spoken to the Paediatric Junior Doctor the Consultant Paediatrician rang the Microbiologist back. The child did indeed have Koplik spots and was now in a side room. The Paediatrician was very apologetic but had spoken to the other parents in the same area as the patient about vaccination history, whilst being careful not to breach confidentiality, and had ascertained that all the other patients and parents were immune. A list of staff had been drawn up and the ward Matron was this very minute talking to Occupational Health… at least the response after the diagnosis was excellent thought the Microbiologist….
 RSS Feed
RSS Feed
