The patient, in his late forties, had a history of chronic Hepatitis C infection resulting in severe liver cirrhosis. He presented with a fever and was very short of breath with a dry cough, which had got progressively worse over 2 weeks. A chest x-ray showed patchy bilateral consolidation more marked in the hilar regions. A diagnosis of severe community acquired pneumonia was made and he was started on IV Co-amoxiclav PLUS IV Clarithromycin. Blood cultures, sputum, HIV test and urine for Legionella and Pneumococcal antigens were sent to the microbiology laboratory but these all failed to identify a cause.
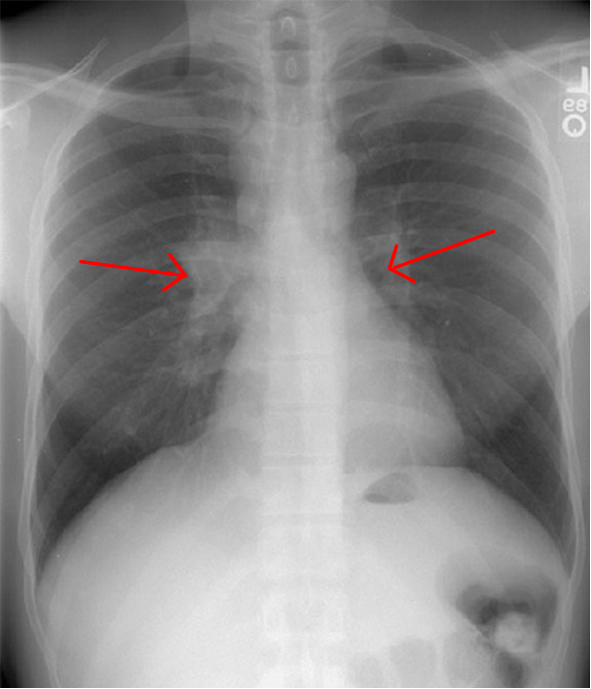
Hilar lymphadenopathy
The patient’s condition was deteriorating; it was felt his severe liver cirrhosis may have rendered him immunocompromised, so he was admitted to the critical care unit for non-invasive ventilation and his antibiotics were broadened to IV Teicoplanin PLUS IV Meropenem PLUS IV Caspofungin, in addition to the IV Clarithromycin. The Team felt this combination should cover all the common and uncommon causes of community acquired pneumonia seen in the UK as well as potential opportunistic infections related to his immunodeficiency e.g. Aspergillosis. Despite this, the patient continued to get worse and was going to require invasive ventilation.
The critical care ward round with the Microbiologist delved further, revealing that the patient had regularly travelled to South Africa to see relatives who had moved there a few years ago. Not yet satisfied, more details were taken revealing that they lived in a rural area and kept chickens. Gosh Microbiologists do like to ask for the details! Anyhow...The patient had last returned from South Africa 4 weeks prior to becoming unwell. This broadened the differential diagnosis to include microorganisms that are not usually seen in the UK. Further tests were sent and the IV Caspofungin was changed to IV AmBisome to cover possible histoplasmosis.
Forty eight hours later the patient was much better and within 5 days he was back on the normal ward requiring minimal oxygen therapy. Ten days after changing to AmBisome his serology results for histoplasmosis came back positive from the reference laboratory.
So what is histoplasmosis?
Histoplasmosis is a fungal infection caused by the dimorphic fungus Histoplasma capsulatum. Infection with H. capsulatum can range from asymptomatic to severe life-threatening infection. It is called a dimorphic fungus because it has two different ways of growing depending on the temperature; at body temperature it grows like yeast whereas at lower temperatures it grows as a mould. It is the mould form which is infectious.
Histoplasma capsulatum is endemic in certain regions of North, Central and South America, but it is also found in Africa and Asia. In North America it is predominantly found in the Ohio and Mississippi River valleys. Bird and bat droppings enhance the growth of the fungus in soil, and human exposure occurs when contaminated sites are disturbed either by strong winds stirring up the dusty soil, or recreational exposure when entering caves where bats have been roosting. There is no person-to-person transmission; infection only occurs after exposure to the mould form.
There are five main clinical forms of histoplasmosis:
How is histoplasmosis diagnosed?
The first step in diagnosing histoplasmosis is to think of it! It is rare in the UK and so can be overlooked. The clues in this case were the travel history, the chest x-ray appearance and his lack of response to Caspofungin which has no activity against H. capsulatum but treats common fungi like Candida spp. and Aspergillus spp. In addition, the patient had failed to respond to the antibiotics for the “usual culprits” which meant he might have something more unusual. In medicine we often say “when you hear hooves think horses not zebras” but sometimes the hooves may actually be a zebra! (especially if your patient has been to Africa).
The critical care ward round with the Microbiologist delved further, revealing that the patient had regularly travelled to South Africa to see relatives who had moved there a few years ago. Not yet satisfied, more details were taken revealing that they lived in a rural area and kept chickens. Gosh Microbiologists do like to ask for the details! Anyhow...The patient had last returned from South Africa 4 weeks prior to becoming unwell. This broadened the differential diagnosis to include microorganisms that are not usually seen in the UK. Further tests were sent and the IV Caspofungin was changed to IV AmBisome to cover possible histoplasmosis.
Forty eight hours later the patient was much better and within 5 days he was back on the normal ward requiring minimal oxygen therapy. Ten days after changing to AmBisome his serology results for histoplasmosis came back positive from the reference laboratory.
So what is histoplasmosis?
Histoplasmosis is a fungal infection caused by the dimorphic fungus Histoplasma capsulatum. Infection with H. capsulatum can range from asymptomatic to severe life-threatening infection. It is called a dimorphic fungus because it has two different ways of growing depending on the temperature; at body temperature it grows like yeast whereas at lower temperatures it grows as a mould. It is the mould form which is infectious.
Histoplasma capsulatum is endemic in certain regions of North, Central and South America, but it is also found in Africa and Asia. In North America it is predominantly found in the Ohio and Mississippi River valleys. Bird and bat droppings enhance the growth of the fungus in soil, and human exposure occurs when contaminated sites are disturbed either by strong winds stirring up the dusty soil, or recreational exposure when entering caves where bats have been roosting. There is no person-to-person transmission; infection only occurs after exposure to the mould form.
There are five main clinical forms of histoplasmosis:
- Asymptomatic - The most common form. Up to 80% of the population from endemic areas have evidence of past exposure to H. capsulatum without a history of any symptoms
- Acute Pulmonary - Ranging from mild symptoms to severe pneumonia and death. Fever with a non-productive cough and hilar lymphadenopathy are characteristic
- Chronic Pulmonary - Progressive infection over months or years with worsening lung function and cavitation. May mimic tuberculosis
- Acute Disseminated - Severe infection with gastrointestinal symptoms, bone marrow invasion, hepatosplenomegaly and lymphadenopathy. Usually seen in infants or immunocompromised patients. Rapidly fatal if not treated
- Chronic Disseminated – Subacute infection over 10-12 months with progressive bone marrow invasion, hepatosplenomegaly and weight loss. Eventually fatal if not treated
How is histoplasmosis diagnosed?
The first step in diagnosing histoplasmosis is to think of it! It is rare in the UK and so can be overlooked. The clues in this case were the travel history, the chest x-ray appearance and his lack of response to Caspofungin which has no activity against H. capsulatum but treats common fungi like Candida spp. and Aspergillus spp. In addition, the patient had failed to respond to the antibiotics for the “usual culprits” which meant he might have something more unusual. In medicine we often say “when you hear hooves think horses not zebras” but sometimes the hooves may actually be a zebra! (especially if your patient has been to Africa).

Once the diagnosis has been considered the normal first line investigation is serology for H. capsulatum antigen. A titre of 1:32 or more is considered positive; higher values mean more fungus e.g. 1:64, 1:128. This test can also be used to monitor the effectiveness of treatment; the numerical value decreases as the amount of antigen or fungus decreases.
Other ways of diagnosing histoplasmosis include the demonstration of fungus in clinical specimens either by histological examination, PCR or even culture (warning: high risk specimen! see below).
Is it safe to process in the laboratory?
Histoplasma capsulatum is a Category 3 microorganism and therefore cultures should only be dealt with in a Category 3 laboratory (in the UK this is the standard used for processing sputum samples). The mould form is infectious and can cause infections in biomedical scientists who inadvertently process these moulds in open areas of the laboratory. Clinical information with the request is critical in protecting laboratory staff from exposure.
But the culture has been processed at 37oC so it will be in the non-infectious yeast form, I hear you say! That may initially be true, but after the plates have been left on the bench or put away to save for a week in case other tests may be required, the fungus will start to grow in its mould form and therefore becomes high risk. Trust me, be careful.
How is histoplasmosis treated?
Fortunately the treatment of histoplasmosis is relatively straight forward although often prolonged. Asymptomatic infection does not require any treatment. However for:
Other ways of diagnosing histoplasmosis include the demonstration of fungus in clinical specimens either by histological examination, PCR or even culture (warning: high risk specimen! see below).
Is it safe to process in the laboratory?
Histoplasma capsulatum is a Category 3 microorganism and therefore cultures should only be dealt with in a Category 3 laboratory (in the UK this is the standard used for processing sputum samples). The mould form is infectious and can cause infections in biomedical scientists who inadvertently process these moulds in open areas of the laboratory. Clinical information with the request is critical in protecting laboratory staff from exposure.
But the culture has been processed at 37oC so it will be in the non-infectious yeast form, I hear you say! That may initially be true, but after the plates have been left on the bench or put away to save for a week in case other tests may be required, the fungus will start to grow in its mould form and therefore becomes high risk. Trust me, be careful.
How is histoplasmosis treated?
Fortunately the treatment of histoplasmosis is relatively straight forward although often prolonged. Asymptomatic infection does not require any treatment. However for:

Click for larger image
If the patient is immunocompromised, and remains so after treatment, then it is recommended that they are given suppression therapy with PO Itraconazole 200mg OD either for the duration of their immunosuppression or lifelong if the immunosuppression is irreversible.
The patient above was treated for acute pulmonary histoplasmosis and made a good recovery. Because he had ongoing severe liver cirrhosis secondary to Hepatitis C it was decided to give him lifelong PO Itraconazole suppression therapy.
Histoplasmosis is rare in the UK but should be considered in any patient with a travel history suggesting possible exposure, who presents with a dry cough and hilar lymphadenopathy, and who doesn’t respond to conventional antibiotic treatment for community acquired pneumonia. I may have a reputation for seeking out weird and wonderful microorganisms in clinical diagnoses but it is only to blog about them!
The patient above was treated for acute pulmonary histoplasmosis and made a good recovery. Because he had ongoing severe liver cirrhosis secondary to Hepatitis C it was decided to give him lifelong PO Itraconazole suppression therapy.
Histoplasmosis is rare in the UK but should be considered in any patient with a travel history suggesting possible exposure, who presents with a dry cough and hilar lymphadenopathy, and who doesn’t respond to conventional antibiotic treatment for community acquired pneumonia. I may have a reputation for seeking out weird and wonderful microorganisms in clinical diagnoses but it is only to blog about them!
 RSS Feed
RSS Feed
