The patient was a middle aged man who was originally born in South America, but who had lived in the UK for a number of years. He made an appointment to see his GP when his wife had noticed that his eyes had started to go yellow. By the time he saw his GP he was clearly jaundiced, although he was not febrile and had no abdominal pain and so infection was not suspected. The GP arranged for some blood tests and an abdominal ultrasound scan to look for any obstruction in the biliary system which might account for the man’s symptoms. The blood tests confirmed a raised bilirubin and slightly abnormal live enzymes, but the total white blood cell count and CRP looked normal. The ultrasound did not show any gallstones (the most common cause of obstruction in the UK other than traffic jams!) but did show a dilated common bile duct which suggested some form of obstruction.

The patient was referred to a Gastroenterologist for further investigation. Having seen the patient the Gastroenterologist wondered if he might have come into contact with some “funny infection” relating to his origin of South America that might be causing the jaundice and abnormal liver enzymes and so called the Microbiologist to discuss the patient.
While on the telephone the Microbiologist scanned through the patients results and whilst the total white blood cells were within the normal range, the small part of this made up of eosinophils, was in fact raised.
“I wonder if this is fascioliasis” said the Microbiologist, “you know a liver fluke”.
“Really?” replied the Gastroenterologist, “you might have fluked the diagnosis, but I’d better ask for an ERCP in the meantime to make sure it isn’t something more sinister like a cancer or something”.
The Gastroenterologist arranged for three stool samples to be sent on consecutive days and also for blood to be taken, and wrote a referral letter for ERCP (Endoscopic Retrograde Cholangio-Pancreatography). In the meantime the lab set to work looking at the poo!
What is a liver fluke?
The liver fluke, Fasciola hepatica, is a trematode parasite normally found in herbivores such as sheep, cattle and water buffalo as well as some fresh water snails. It is apparently found on every continent except Antarctica.
Herbivores pass eggs in their faeces which develop in fresh water into larvae in about 2 weeks. The larvae then infect fresh water snails where large numbers of more mature free living larvae are produced and excreted back into the water. These free living larvae then attach to water plants where they encyst, known as metacercariae, which helps them survive if the plant dries out. Humans become infected after drinking water or eating water plants contaminated with metacercariae e.g. water cress. There is no person-to-person transmission.
The mature fluke is usually about 10-15mm wide and 30mm long, although there is a less common species Fasciola gigantica which can grow up to 75mm long!
While on the telephone the Microbiologist scanned through the patients results and whilst the total white blood cells were within the normal range, the small part of this made up of eosinophils, was in fact raised.
“I wonder if this is fascioliasis” said the Microbiologist, “you know a liver fluke”.
“Really?” replied the Gastroenterologist, “you might have fluked the diagnosis, but I’d better ask for an ERCP in the meantime to make sure it isn’t something more sinister like a cancer or something”.
The Gastroenterologist arranged for three stool samples to be sent on consecutive days and also for blood to be taken, and wrote a referral letter for ERCP (Endoscopic Retrograde Cholangio-Pancreatography). In the meantime the lab set to work looking at the poo!
What is a liver fluke?
The liver fluke, Fasciola hepatica, is a trematode parasite normally found in herbivores such as sheep, cattle and water buffalo as well as some fresh water snails. It is apparently found on every continent except Antarctica.
Herbivores pass eggs in their faeces which develop in fresh water into larvae in about 2 weeks. The larvae then infect fresh water snails where large numbers of more mature free living larvae are produced and excreted back into the water. These free living larvae then attach to water plants where they encyst, known as metacercariae, which helps them survive if the plant dries out. Humans become infected after drinking water or eating water plants contaminated with metacercariae e.g. water cress. There is no person-to-person transmission.
The mature fluke is usually about 10-15mm wide and 30mm long, although there is a less common species Fasciola gigantica which can grow up to 75mm long!

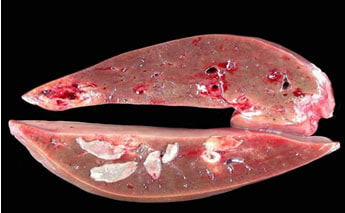
Those big white bits are the flukes!
How does fascioliasis present?
There are two phases of infection with Fasciola hepatica.
The acute phase occurs 4-7 days after exposure and lasts from a few weeks to several months. During this period larvae penetrate through the gastrointestinal wall and migrate to the liver where they can cause a transient hepatitis. Patients can be asymptomatic or present with fever, malaise, nausea, vomiting, diarrhoea, weight loss and abdominal pain. The liver is often slightly enlarged (hepatomegaly) and the liver enzymes and eosinophils can be raised.
The chronic phase occurs 3-4 months after exposure when the larvae mature in to flukes in the bile ducts and start to produce eggs. This can be asymptomatic but can also present many years later with similar symptoms as the acute phase as well as biliary colic (pain) and obstructive jaundice.
How is fascioliasis diagnosed?
The most common method for diagnosing fascioliasis is the detection of eggs in stool samples from infected patients, although these are only present in the chronic phase. It is best to test 3 samples on consecutive days to give the laboratory the best chance of seeing the eggs. It is possible to get caught out when seeing eggs in stool as there is a situation known as “pseudo-fascioliasis” when eggs are seen in the stool after the ingestion of liver from an infected animal. These eggs are not infectious (remember only the mature larvae are infective) so a careful dietary history is important before taking the samples.
There are two phases of infection with Fasciola hepatica.
The acute phase occurs 4-7 days after exposure and lasts from a few weeks to several months. During this period larvae penetrate through the gastrointestinal wall and migrate to the liver where they can cause a transient hepatitis. Patients can be asymptomatic or present with fever, malaise, nausea, vomiting, diarrhoea, weight loss and abdominal pain. The liver is often slightly enlarged (hepatomegaly) and the liver enzymes and eosinophils can be raised.
The chronic phase occurs 3-4 months after exposure when the larvae mature in to flukes in the bile ducts and start to produce eggs. This can be asymptomatic but can also present many years later with similar symptoms as the acute phase as well as biliary colic (pain) and obstructive jaundice.
How is fascioliasis diagnosed?
The most common method for diagnosing fascioliasis is the detection of eggs in stool samples from infected patients, although these are only present in the chronic phase. It is best to test 3 samples on consecutive days to give the laboratory the best chance of seeing the eggs. It is possible to get caught out when seeing eggs in stool as there is a situation known as “pseudo-fascioliasis” when eggs are seen in the stool after the ingestion of liver from an infected animal. These eggs are not infectious (remember only the mature larvae are infective) so a careful dietary history is important before taking the samples.

In the acute phase, before the eggs are present in stool, serology can be done to look for antibodies indicating an immune response to the infection. This can also be done in the chronic phase but it is important to remember that people from an endemic country can have positive serology if they have been infected and treated in the past.
How is fascioliasis treated?
The mainstay of treatment for fascioliasis is a drug called Triclabendazole, given as a one off 10mg/kg dose. This is not licensed for use in humans in the UK and would have to be got on a named-patient basis. I could find over 40 different Triclabendazole products listed on the Internet for the treatment of liver flukes but unfortunately these are all for use in animals! I could only find one product for use in humans, called Egaten and made by Novartis.
Needless to say with so many products available for animals and the widespread use of Triclabendazole to treat liver flukes in sheep and cattle around the world, there is now an increasing problem with Triclabendazole resistance in liver flukes.
An alternative agent which may be effective in the treatment of fascioliasis is another named-patient only drug called Nitazoxanide. This drug is used to treat other parasitic diseases in humans such as cryptosporidiosis and giardiasis, so it is known to be safe in humans. The only problem is that there is no clear evidence that it does work, it’s just theoretical. Again, there are many products for use in animals to treat parasitic diseases so resistance might also be a problem with Nitazoxanide as well! It’s a difficult situation.
There are calls to reduce the number of drugs used in animal husbandry but on the other hand we don’t want animals suffering from infections, and when we buy meat or pâté in supermarkets nobody wants to eat a plate of liver and find half a liver fluke left on their plate! Gross!!!! Umm this isn’t meant as a promotion for meat free January or Veganary as it is being called…but…
How is fascioliasis treated?
The mainstay of treatment for fascioliasis is a drug called Triclabendazole, given as a one off 10mg/kg dose. This is not licensed for use in humans in the UK and would have to be got on a named-patient basis. I could find over 40 different Triclabendazole products listed on the Internet for the treatment of liver flukes but unfortunately these are all for use in animals! I could only find one product for use in humans, called Egaten and made by Novartis.
Needless to say with so many products available for animals and the widespread use of Triclabendazole to treat liver flukes in sheep and cattle around the world, there is now an increasing problem with Triclabendazole resistance in liver flukes.
An alternative agent which may be effective in the treatment of fascioliasis is another named-patient only drug called Nitazoxanide. This drug is used to treat other parasitic diseases in humans such as cryptosporidiosis and giardiasis, so it is known to be safe in humans. The only problem is that there is no clear evidence that it does work, it’s just theoretical. Again, there are many products for use in animals to treat parasitic diseases so resistance might also be a problem with Nitazoxanide as well! It’s a difficult situation.
There are calls to reduce the number of drugs used in animal husbandry but on the other hand we don’t want animals suffering from infections, and when we buy meat or pâté in supermarkets nobody wants to eat a plate of liver and find half a liver fluke left on their plate! Gross!!!! Umm this isn’t meant as a promotion for meat free January or Veganary as it is being called…but…

Gourmet liver sandwich... would you like flukes with that?!
So the patient had stool samples sent to the laboratory and the Biomedical Scientist saw parasite eggs. These were confirmed as Fasciola hepatica; the serology also confirmed the diagnosis. The patient was treated with Triclabendazole obtained from Novartis. To ensure there was nothing else going on, the patient had an ERCP which confirmed no other problems. After a few weeks the patient’s jaundice had completely resolved.
The case was presented at the hospital Grand Round at lunchtime and funnily enough there were a lot of plates of partly eaten food left at the end… it would appear it is only Microbiologists who are not put off eating by these types of stories!
The case was presented at the hospital Grand Round at lunchtime and funnily enough there were a lot of plates of partly eaten food left at the end… it would appear it is only Microbiologists who are not put off eating by these types of stories!
 RSS Feed
RSS Feed
